The market access landscape for ultra-orphan biologics is facing its most significant challenge to date. On June 27, 2026, the seven-year orphan drug exclusivity for Alexion Pharmaceuticals' (AstraZeneca) blockbuster biological product Soliris (eculizumab, BLA 125166) in neuromyelitis optica spectrum disorder (NMOSD) officially expired. This milestone removes the final indication-specific labeling barrier for eculizumab biosimilars, allowing developers to update their labels and actively promote their products to the high-volume NMOSD prescriber base.
For specialty pharmacy directors, commercial payer teams, and hospital system procurement managers, the post-exclusivity market represents a crucial case study in specialty drug management. This analysis compares the approved U.S. eculizumab biosimilars—Amgen’s interchangeable Bkemv and Samsung Bioepis/Teva’s Epysqli—and details the Medicare Part B reimbursement economics (HCPCS J1299 for reference Soliris, with biosimilar Q-codes) and real-world payer step-therapy policies shaping biosimilar switching.
Short Answer
Soliris (eculizumab) lost its final labeling defense when its NMOSD orphan drug exclusivity expired on June 27, 2026. This allows the two approved U.S. eculizumab biosimilars to update their FDA labels to include NMOSD, eliminating the "skinny labels" they operated under since launching in early 2025.
These two biosimilars compete on different commercial value propositions:
- Bkemv (eculizumab-aeeb, Amgen, BLA 761333): Approved May 28, 2024 as the first interchangeable biosimilar (its interchangeability exclusivity expired November 28, 2025). It launched in March 2025 at a 10% WAC discount ($5,870.70 per 300 mg vial vs. Soliris's WAC of $6,523).
- Epysqli (eculizumab-aagh, Samsung Bioepis/Teva, BLA 761340): Approved July 19, 2024 as a biosimilar (non-interchangeable at launch). It launched in April 2025 at a 30% WAC discount ($4,566.00 per vial).
Unlike small-molecule generics, eculizumab is physician-administered and is completely absent from CMS retail pharmacy NADAC pricing. Instead, it is reimbursed under Medicare Part B—reference Soliris under HCPCS code J1299 (Injection, eculizumab, 2 mg), with the biosimilars billed under their own codes (Q5152 for Bkemv and Q5151 for Epysqli)—on an Average Sales Price (ASP) + 6% buy-and-bill framework. Commercial payers are driving rapid adoption by implementing restrictive step-therapy edits. For example, Blue Shield of California requires patients with NMOSD to try Bkemv or Epysqli before covering brand-name Soliris, effective February 1, 2026.
Eculizumab Product Profiles: Reference vs. Biosimilars
To understand the competitive dynamics in the complement-inhibitor space, we must compare the clinical and pricing profiles of the three licensed eculizumab formulations.
Product Matrix
| Brand Name | Proper Name (BLA Number) | BLA Type | FDA Approval Date | Interchangeability Status | WAC Price Per Vial (300 mg) | Launch Date | Labeled Indications (as of July 2026) |
|---|---|---|---|---|---|---|---|
| Soliris | eculizumab (BLA 125166) | Reference Product (351(a)) | March 16, 2007 | Reference Product | $6,523.00 | March 2007 | PNH, aHUS, gMG, NMOSD |
| Bkemv | eculizumab-aeeb (BLA 761333) | Biosimilar (351(k)) | May 28, 2024 | Interchangeable | $5,870.70 (10% discount) | March 2025 | PNH, aHUS, gMG, NMOSD (updated post-June 27) |
| Epysqli | eculizumab-aagh (BLA 761340) | Biosimilar (351(k)) | July 19, 2024 | Biosimilar (Not interchangeable) | $4,566.00 (30% discount) | April 2025 | PNH, aHUS, gMG, NMOSD (updated post-June 27) |
Interchangeability and the Substitution Lever
Amgen’s Bkemv holds the distinction of being the first FDA-approved interchangeable eculizumab biosimilar. Under the Biologics Price Competition and Innovation Act (BPCIA), an interchangeable designation allows a pharmacist to substitute the biosimilar for the reference product without the intervention of the prescribing healthcare provider, subject to state-level pharmacy laws.
However, because eculizumab is an intravenous infusion administered in outpatient clinics or hospital infusion centers rather than a retail pharmacy product, the utility of pharmacy-level substitution is limited. Instead, interchangeability serves as a clinical reassurance for physicians and hospital pharmacy directors making formulary decisions, helping to overcome the "nocebo effect" when transitioning patients off Soliris.
Samsung Bioepis and Teva’s Epysqli was approved as a standard biosimilar (non-interchangeable). To offset the lack of interchangeable status, Samsung Bioepis introduced a significantly lower Wholesale Acquisition Cost (WAC) price. Epysqli's WAC of $4,566.00 represents a 30% discount compared to Soliris, making it highly attractive to hospital systems operating under capitated budgets or payers trying to minimize overall specialty drug spend.
Biological Target and Mechanism of Action
Eculizumab is a recombinant humanized monoclonal IgG2/4 kappa antibody designed to selectively target the complement system. The complement system is a key arm of the innate immune response, consisting of a cascade of serum proteins that help destroy invading pathogens. However, in certain rare diseases, dysregulated complement activation leads to severe systemic pathology.
The C5 Cleavage Block
The mechanism of action for eculizumab relies on high-affinity binding to the C5 complement protein. Specifically:
- Binding Event: Eculizumab binds to the alpha chain of the C5 protein, preventing its cleavage by C5 convertase enzymes into two active fragments: C5a and C5b.
- Inhibition of C5a: By blocking the release of C5a (a highly potent anaphylatoxin), eculizumab reduces inflammatory cell recruitment, mast cell degranulation, and endothelial cell activation.
- Inhibition of C5b and MAC Assembly: By blocking the generation of C5b, eculizumab prevents the subsequent binding of complement proteins C6, C7, C8, and C9. These proteins ordinarily self-assemble on cell membranes to form the Membrane Attack Complex (MAC), also known as the terminal complement complex C5b-9.
Disease-Specific Effects of MAC Blockade
In the four labeled indications, blocking MAC assembly halts the primary driver of tissue damage:
- In PNH: It prevents the complement-mediated lysis of red blood cells that lack protective surface proteins (CD55 and CD59), reducing chronic intravascular hemolysis.
- In aHUS: It halts the activation of platelets and endothelial cell injury in the microvasculature, preventing thrombotic microangiopathy (TMA) and subsequent renal failure.
- In gMG: It prevents MAC-mediated destruction of the post-synaptic neuromuscular junction membrane, preserving acetylcholine receptor availability and muscle signaling.
- In NMOSD: It prevents complement-mediated astrocytic injury and demyelination in the central nervous system driven by autoantibodies targeting the aquaporin-4 water channel.
Clinical Indications and Trial Context
Eculizumab is indicated for four distinct high-cost clinical conditions, each with its own patient population and dosing requirements:
1. Paroxysmal Nocturnal Hemoglobinuria (PNH)
PNH is a rare, life-threatening blood disease characterized by complement-mediated destruction of red blood cells (hemolysis). The pivotal clinical trials demonstrating Soliris's efficacy included the TRIUMPH study (a randomized, double-blind, placebo-controlled Phase III trial) and the SHEPHERD study (an open-label safety trial).
Dosing for PNH involves an induction phase (600 mg intravenously weekly for 4 weeks) followed by a maintenance phase of 900 mg intravenously every 2 weeks.
2. Atypical Hemolytic Uremic Syndrome (aHUS)
aHUS is a chronic disease characterized by complement-mediated thrombotic microangiopathy (TMA), which leads to systemic blood clot formation and acute kidney failure. The approval was supported by prospective open-label trials in adult and pediatric patients showing significant improvements in platelet count and renal function.
Dosing for aHUS requires higher doses: an induction phase (900 mg weekly for 4 weeks) followed by a maintenance phase of 1,200 mg intravenously every 2 weeks.
3. Generalized Myasthenia Gravis (gMG)
gMG is a chronic autoimmune neuromuscular disease characterized by muscle weakness. Eculizumab is indicated for patients who are anti-acetylcholine receptor (AChR) antibody positive, representing roughly 85% of all gMG patients. The pivotal Phase III REGAIN trial and its open-label extension demonstrated significant reductions in muscle weakness and improvements in activities of daily living.
The maintenance dose is 1,200 mg intravenously every 2 weeks, matching the aHUS schedule.
4. Neuromyelitis Optica Spectrum Disorder (NMOSD)
NMOSD is a rare autoimmune disease of the central nervous system that primarily attacks the optic nerves and spinal cord, leading to blindness and paralysis. Eculizumab is approved strictly for patients who are anti-aquaporin-4 (AQP4) antibody positive. The pivotal Phase III PREVENT trial demonstrated a 94% reduction in the risk of relapse compared to placebo over a median treatment period of 48 weeks.
Maintenance dosing matches the gMG/aHUS schedule of 1,200 mg every 2 weeks. Because relapses in NMOSD can cause permanent disability, relapse prevention is the primary clinical goal.
The Expiration of Soliris’s NMOSD Orphan Exclusivity
The June 27, 2026 expiration of Soliris’s orphan drug exclusivity for NMOSD is the most critical regulatory event in this drug class since initial biosimilar approvals.
The Section viii Labeling Carve-Out
Prior to June 27, 2026, both Bkemv and Epysqli launched under "skinny labels" using Section viii statements to carve out the protected NMOSD indication. This occurred because Soliris held a seven-year orphan drug exclusivity for the treatment of neuromyelitis optica spectrum disorder in adult patients who are anti-aquaporin-4 (AQP4) antibody positive.
While the biosimilars were approved for Paroxysmal Nocturnal Hemoglobinuria (PNH) and Atypical Hemolytic Uremic Syndrome (aHUS), and later added Generalized Myasthenia Gravis (gMG) after Soliris’s gMG exclusivity expired in October 2024, they were legally blocked from listing NMOSD. This restricted their clinical marketing. Prescribers could theoretically use the biosimilars "off-label" for NMOSD, but payers were reluctant to cover off-label Rare Disease biologics, and manufacturers were legally prohibited from promoting them for this indication.
Post-Exclusivity Label Updates
With the expiration of the exclusivity, Amgen and Samsung Bioepis submitted labeling supplements to the FDA to include the NMOSD indication. This label expansion is expected to result in:
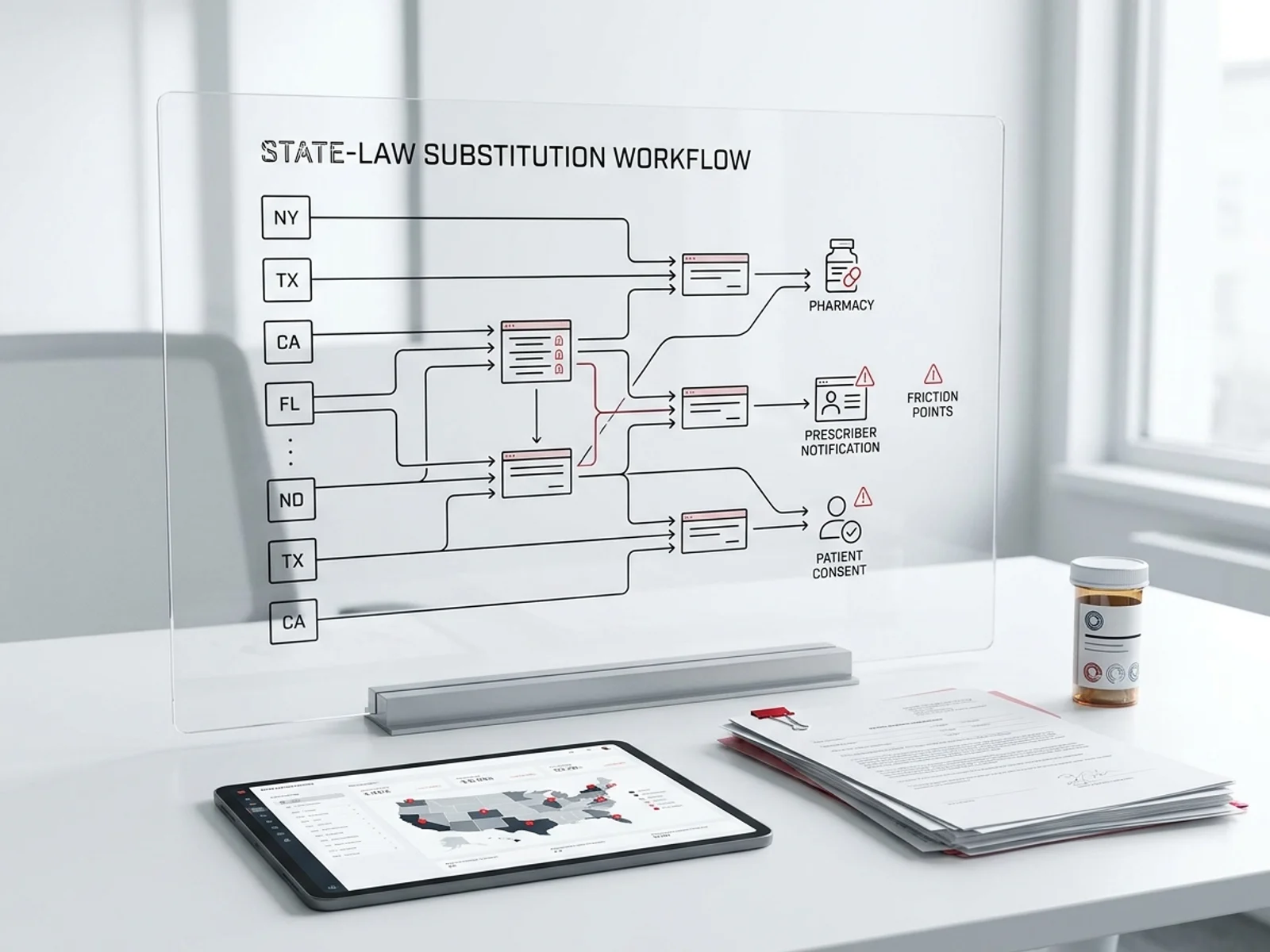
- Direct Promotion: Biosimilar sales representatives can actively market Bkemv and Epysqli to neurologists treating NMOSD, using head-to-head biosimilarity data.
- State Law Alignment: In states that mandate that biosimilars match the exact labeled indications of the reference product to qualify for automatic substitution, interchangeable Bkemv now fully meets the criteria for NMOSD patients.
- Payer Policy Revision: Payers can update their medical benefit criteria to mandate biosimilar use for NMOSD, eliminating the administrative exception processes previously required for skinny-labeled products.
The ULTOMIRIS and SOLIRIS REMS Program
Because eculizumab inhibits the terminal complement pathway, it prevents the body from fighting encapsulated bacteria. This creates a Boxed Warning for serious, life-threatening meningococcal infections. To manage this clinical risk, the FDA mandates a Risk Evaluation and Mitigation Strategy (REMS) program.
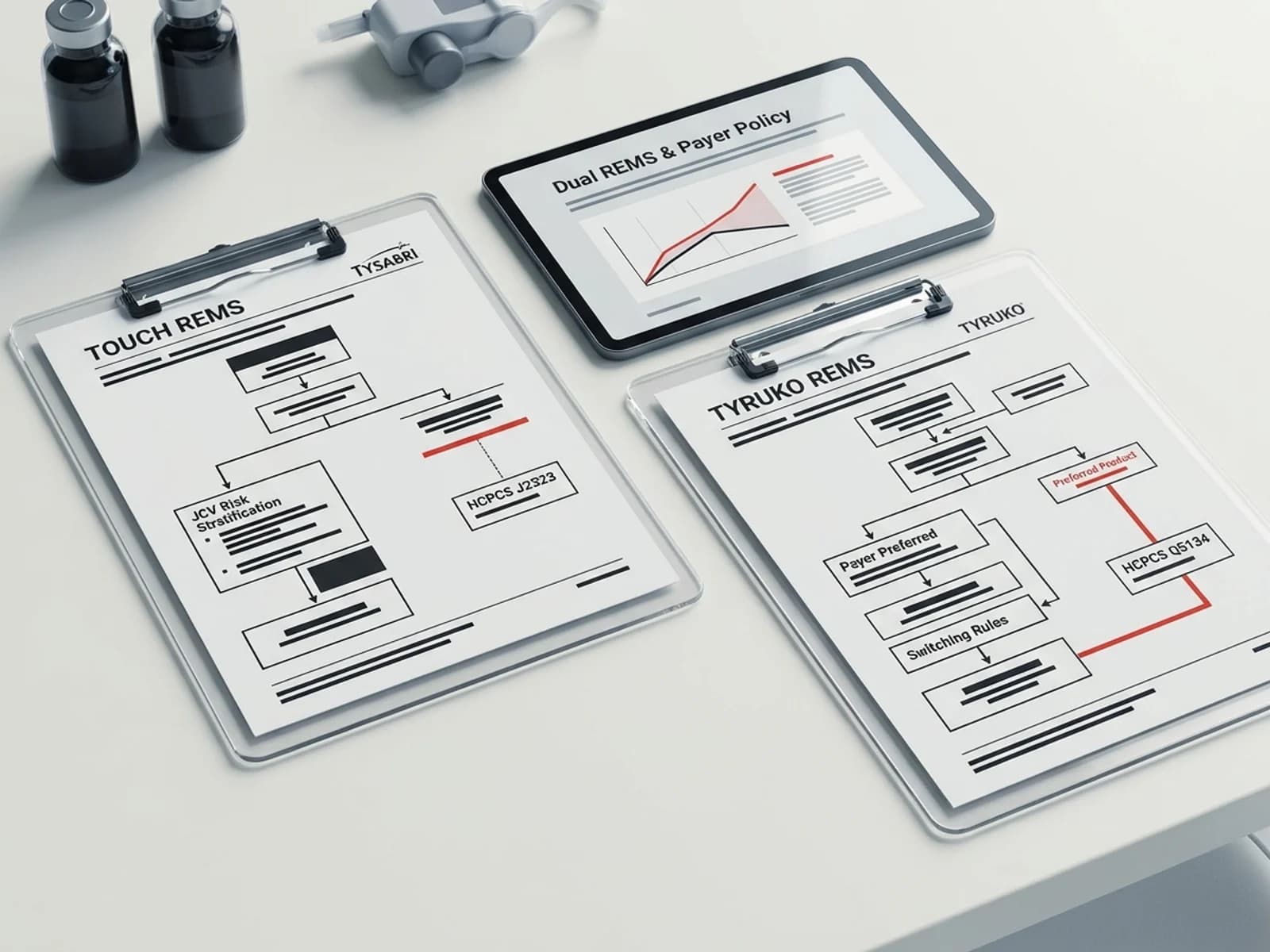
Key Requirements of the Shared REMS
Rather than maintaining separate programs, the FDA approved a single, shared system called the ULTOMIRIS and SOLIRIS REMS. This shared infrastructure includes both reference biologics (Soliris and Ultomiris) and their biosimilars (Bkemv and Epysqli).
The REMS mandates several strict compliance loops:
- Prescriber Certification: Clinicians must enroll in the REMS, pass an educational assessment, and sign an agreement to counsel patients on the risk of meningococcal infection.
- Meningococcal Vaccination: Patients must receive meningococcal vaccines (both MenACWY conjugate and MenB serogroup B vaccines) at least two weeks prior to receiving the first dose of eculizumab. If urgent therapy is required before the two weeks have passed, the patient must be prescribed two weeks of prophylactic antibiotics.
- Patient Safety Card: Patients must carry a physical safety card outlining the symptoms of meningococcal infection (severe headache, fever, stiff neck, photophobia) to show to emergency medical personnel.
- Pharmacy Certification: Dispensing specialty pharmacies must verify prescriber certification and active patient vaccination records before releasing the drug.
Required Meningococcal Vaccination Protocols
The shared REMS mandates adherence to specific Advisory Committee on Immunization Practices (ACIP) guidelines. The following table summarizes the required vaccination schedules:
| Vaccine Category | Specific Target Serogroups | Recommended Vaccine Products | Dosing Schedule for Adults | REMS Compliance Loop |
|---|---|---|---|---|
| MenACWY Conjugate | Serogroups A, C, W, and Y | Menveo, MenQuadfi | Primary series: 2 doses administered 8-12 weeks apart; booster dose every 5 years if treatment continues. | Must be documented in the patient registry; requires a 2-week wait post-dose or antibiotic cover. |
| MenB (Serogroup B) | Serogroup B | Bexsero, Trumenba | Bexsero: 2-dose series (0, 1 month apart). Trumenba: 3-dose series (0, 1-2, 6 months) or 2-dose series. | Must be completed; note that Bexsero and Trumenba are not interchangeable. |
Note: In case of delayed vaccination, clinicians must prescribe a prophylactic antibiotic (such as penicillin, ciprofloxacin, or erythromycin) for at least two weeks following the initial vaccine dose.
Reimbursement Economics: Medical Benefit Buy-and-Bill and ASP
A key error in DOAC or oncology-market access planning is applying retail pharmacy pricing rules to physician-administered biologics. Eculizumab is reimbursed under the medical benefit, not the pharmacy benefit.
The Absence of Eculizumab in NADAC
In our analysis of the CMS National Average Drug Acquisition Cost (NADAC) database, eculizumab and Soliris return zero rows. Retail pharmacies do not carry or dispense Soliris; it is distributed through specialty distributors directly to clinics, hospitals, and specialized infusion centers. Consequently, retail pharmacy acquisition metrics do not apply.
The Buy-and-Bill and ASP+6% Framework
Eculizumab is reimbursed under Medicare Part B. Reference Soliris is billed using HCPCS code J1299 (Injection, eculizumab, 2 mg), while the biosimilars carry their own product-specific codes—Q5152 (Injection, eculizumab-aeeb (Bkemv), biosimilar, 2 mg) and Q5151 (Injection, eculizumab-aagh (Epysqli), biosimilar, 2 mg). Outpatient providers purchase the drug through specialty distributors, administer the infusion to the patient, and bill Medicare or commercial insurers using the applicable code. (Note: Soliris previously billed under the now-superseded J1300 at a 10 mg basis; current claims use the 2 mg J1299 and biosimilar Q-codes.)
Under Medicare Part B, the reimbursement is based on the Average Sales Price (ASP) plus a 6% administration fee (reduced to 4.3% under sequestration). The ASP is calculated quarterly by the FDA and CMS based on manufacturer-reported transaction data, factoring in all commercial discounts, rebates, and chargebacks.
The ASP Lag and "Buy-and-Bill" Risk
Because ASP is calculated retrospectively based on data from two quarters prior, there is a six-month lag in reimbursement rates. This lag creates distinct commercial dynamics during biosimilar launches:
- The "Reimbursement Cliff": When a lower-priced biosimilar launches, the reference product's ASP remains high for two quarters. During this time, providers can buy the cheaper biosimilar but bill at the higher brand-based J-code rate, temporarily capturing a wider margin.
- The "Price Compression": As biosimilar market share increases, the weighted average ASP for the J-code code falls. Providers who continue to purchase brand-name Soliris at WAC will face negative margins (under-reimbursement), forcing them to switch to the cheaper biosimilar.
Financial Exposure and Billing Risk Management
For a hospital or independent infusion clinic, managing a patient on maintenance eculizumab (dosed at 1,200 mg, or four 300 mg vials, every 2 weeks) represents a significant financial commitment. The clinic must purchase $26,092 worth of drug product every 14 days per patient.
Key risk factors include:
- Administrative Delays: A prior authorization renewal delay can cause a gap in coverage, leaving the clinic with a massive unpaid inventory bill.
- Wasted Product: If a patient misses an infusion appointment after the vial has been reconstituted, the clinic may absorb the full product cost.
- Double Billing Errors: Coding errors in HCPCS units (J1299 and the biosimilar Q-codes are billed at 1 unit per 2 mg; therefore, a 1,200 mg dose equals 600 units) can result in immediate claim rejections.
This extreme financial exposure drives providers to align their purchasing closely with payer-preferred formularies and biosimilar lists.
Payer Step-Therapy Policies: Shifting the Market
Because eculizumab is an expensive specialty drug—costing between $450,000 and $600,000 per patient annually depending on dosing—payers are actively intervening to enforce biosimilar switching.
Blue Shield of California's Medication Policy
A prime example of active payer management is Blue Shield of California. In its medical benefit drug policies, the payer has implemented strict step-therapy edits for eculizumab:
- Step Criteria: Effective February 1, 2026, for the NMOSD indication, and December 1, 2025, for the gMG indication, Blue Shield of California requires patients to try one of the preferred eculizumab biosimilars (Bkemv or Epysqli) before brand-name Soliris will be approved.
- Grandfathering Policies: Unlike chronic cardiovascular drugs where patients are rarely switched, payers are increasingly implementing "active switch" programs for stable eculizumab patients. If a patient is stable on Soliris, the payer may mandate a transition to Bkemv or Epysqli at the next authorization renewal cycle, unless the prescriber documents a clinical contraindication or an intolerable side effect to the biosimilar.
- Widespread Life Coverage: Samsung Bioepis reported that Epysqli achieved 94% commercial and Medicare lives coverage in the U.S. as of June 9, 2026. This rapid coverage expansion demonstrates that payers are actively prioritizing the 30% WAC discount to reduce specialty drug spending.
The Ultomiris Transition Barrier
Despite aggressive payer step-therapy for eculizumab, the overall eculizumab biosimilar market size is constrained by Alexion’s lifecycle management. Alexion successfully converted over 60% of Soliris patients to Ultomiris (ravulizumab-cwvz), which requires infusions only every 8 weeks compared to Soliris's 2-week interval.
Because Ultomiris holds its own orphan drug exclusivities extending into the 2030s (its NMOSD approval was granted on March 25, 2024), eculizumab biosimilars cannot be substituted for Ultomiris. Payers must decide whether to mandate step-therapy requiring patients to fail eculizumab biosimilars before accessing Ultomiris, or if they will allow direct access to Ultomiris due to its superior clinical convenience and reduced infusion costs.
Differentiating the Eculizumab Regulatory History
To maintain editorial clarity, it is important to distinguish this analysis from previous publications on eculizumab. Our earlier piece, Soliris NMOSD Exclusivity Expiration: Skinny Label & REMS Barriers for Bkemv (published June 21, 2026), served as a regulatory preview focusing on the theoretical mechanics of the Section viii skinny label and the administrative structure of the shared REMS database.
This current analysis focuses on the post-expiration commercial reality: the actual launch pricing, the specific Part B J-code reimbursement economics (J1299 and the biosimilar Q-codes), and the concrete 2026 payer step-therapy policies (such as Blue Shield of California's) that are driving real-world biosimilar switching. For the broader interchangeable-biosimilar landscape, see our interchangeable biosimilars by the numbers analysis.
Frequently Asked Questions (FAQ)
What indication did Soliris lose exclusivity for on June 27, 2026?
Soliris lost orphan drug exclusivity for the treatment of Neuromyelitis Optica Spectrum Disorder (NMOSD) in adult patients who are anti-aquaporin-4 (AQP4) antibody positive. This was the final indication-specific exclusivity barrier listed in the FDA Purple Book.
How do Bkemv and Epysqli differ in their FDA designations?
Amgen's Bkemv is approved as an interchangeable biosimilar to Soliris, meaning it can be substituted at the pharmacy level without prescriber intervention in states where laws allow. Samsung Bioepis/Teva's Epysqli is approved as a standard biosimilar (non-interchangeable), relying on a deeper 30% WAC discount to secure market share.
Why is eculizumab missing from the CMS NADAC database?
Eculizumab is physician-administered via intravenous infusion and is distributed through specialty distributors directly to clinics and hospitals. Because it is not dispensed by retail pharmacies under a pharmacy benefit, it has no retail acquisition cost history and does not appear in the retail-focused NADAC database.
How is eculizumab reimbursed under Medicare Part B?
Reference Soliris is reimbursed under HCPCS code J1299 (Injection, eculizumab, 2 mg), while the biosimilars use Q5152 (Bkemv) and Q5151 (Epysqli), based on the Average Sales Price (ASP) plus a 6% administration fee. The ASP is updated quarterly by CMS based on historical manufacturer transaction data, incorporating all discounts and rebates.
What step-therapy policies are payers implementing for Soliris?
Major payers, including Blue Shield of California, have introduced policies requiring patients to try and fail preferred eculizumab biosimilars (Bkemv or Epysqli) before brand-name Soliris will be covered. These step-therapy rules became effective for gMG in late 2025 and for NMOSD in February 2026.
Why does the NMOSD orphan exclusivity matter if biosimilars already launched for PNH and aHUS?
NMOSD represents a significant portion of eculizumab's clinical volume. While biosimilars were approved for PNH and aHUS, they had to carve out NMOSD from their labels. Prescribers could not be marketed to, and pharmacies could not automatically substitute for NMOSD. The expiration of this exclusivity allows biosimilars to expand their approved labels, enabling active clinical promotion and pharmacy-level substitution.
How does the eculizumab J-code unit calculation work for billing?
The reference code J1299 (and the biosimilar Q-codes Q5152 and Q5151) represents 2 mg of eculizumab per unit. Because a standard maintenance dose is 1,200 mg, the provider must submit a claim for exactly 600 units per infusion. Failure to calculate this unit ratio correctly is a common source of claim denials.
Sources
- U.S. Food and Drug Administration (FDA). Orphan Drug Designations and Approvals Database. Eculizumab (Soliris) NMOSD orphan exclusivity record (Designation date: 2013; Exclusivity end date: June 27, 2026). https://www.accessdata.fda.gov/scripts/opdlisting/oopd/detailedIndex.cfm?cfgridkey=398713
- U.S. Food and Drug Administration (FDA). Approved Licensed Biological Products with Biosimilarity and Interchangeability Evaluations (Purple Book). Licensed biologics: Soliris (BLA 125166), Bkemv (BLA 761333), Epysqli (BLA 761340) records. https://purplebooksearch.fda.gov/
- Centers for Medicare & Medicaid Services (CMS). Medicare Part B Drug Pricing Files and Billing and Coding: Eculizumab and Biosimilars (A54548). HCPCS J1299 (eculizumab), Q5152 (Bkemv), and Q5151 (Epysqli) Average Sales Price (ASP) rates, Q1 and Q2 2026. https://www.cms.gov/medicare/payment/part-b-drug-average-sales-price
- Blue Shield of California. Medication Policy — eculizumab (Bkemv, Epysqli, Soliris). Medical benefit drug policy, revised February 2026. https://www.blueshieldca.com/content/dam/bsca/en/provider/docs/medi-cal-med-benefit-drug-policy/eculizumab-MCAL-UMRx-provider.pdf
- Samsung Bioepis. Samsung Bioepis Corporate Coverage Update, June 9, 2026. Lives-covered data for Epysqli (eculizumab-aagh) launch. https://www.samsungbioepis.com/en/newsroom/newsroomDetail.do?idx=392
Disclaimer: This article provides independent regulatory and market access analysis for biopharma professionals and does not constitute clinical, medical, or legal advice.