The AIDS Institute's February 2026 report, "Shortchanged," documented a scenario where a copay accumulator nearly doubled the amount a plan collected from a single patient's specialty drug — from $8,550 to $15,160 — by preventing manufacturer copay assistance from counting toward the patient's out-of-pocket maximum. The ASHP specialty pharmacy guide on navigating copay adjustment programs confirmed that these programs create unexpected out-of-pocket expenses for patients and strain pharmacy operations.
Twenty-six states plus the District of Columbia and Puerto Rico have passed laws restricting copay accumulator programs. Federal rules currently allow accumulators except when a generic equivalent exists. The NAIC Prescription Drug Coverage Working Group reported in early 2026 that as of late 2025, 43% of commercially insured beneficiaries were enrolled in plans with copay accumulators. Yet patients routinely discover their plan has an accumulator only after their copay assistance is exhausted mid-year and they face the full cost-sharing obligation from zero.
This article covers the appeal workflow for patients and provider teams navigating copay accumulator decisions — what plan document evidence to gather, what ERISA and state law protections apply, when patient assistance still does not count, and how to structure the appeal.
Understanding what is being appealed
The accumulator is not a claim denial
A copay accumulator is not a traditional claim denial. The prescription is filled, the copay card is processed, and the patient pays nothing at the counter. What changes is invisible: the copay assistance does not count toward the patient's deductible or annual out-of-pocket maximum. The patient only discovers the problem when the copay card runs out mid-year and they face the full cost-sharing obligation.
This distinction matters for appeals because:
- The plan may not have issued a formal adverse determination letter that triggers appeal rights
- The patient may not realize they have been harmed until months after the accumulator was applied
- The appeal may need to challenge the plan design rather than a specific claim decision
Identifying which program is in effect
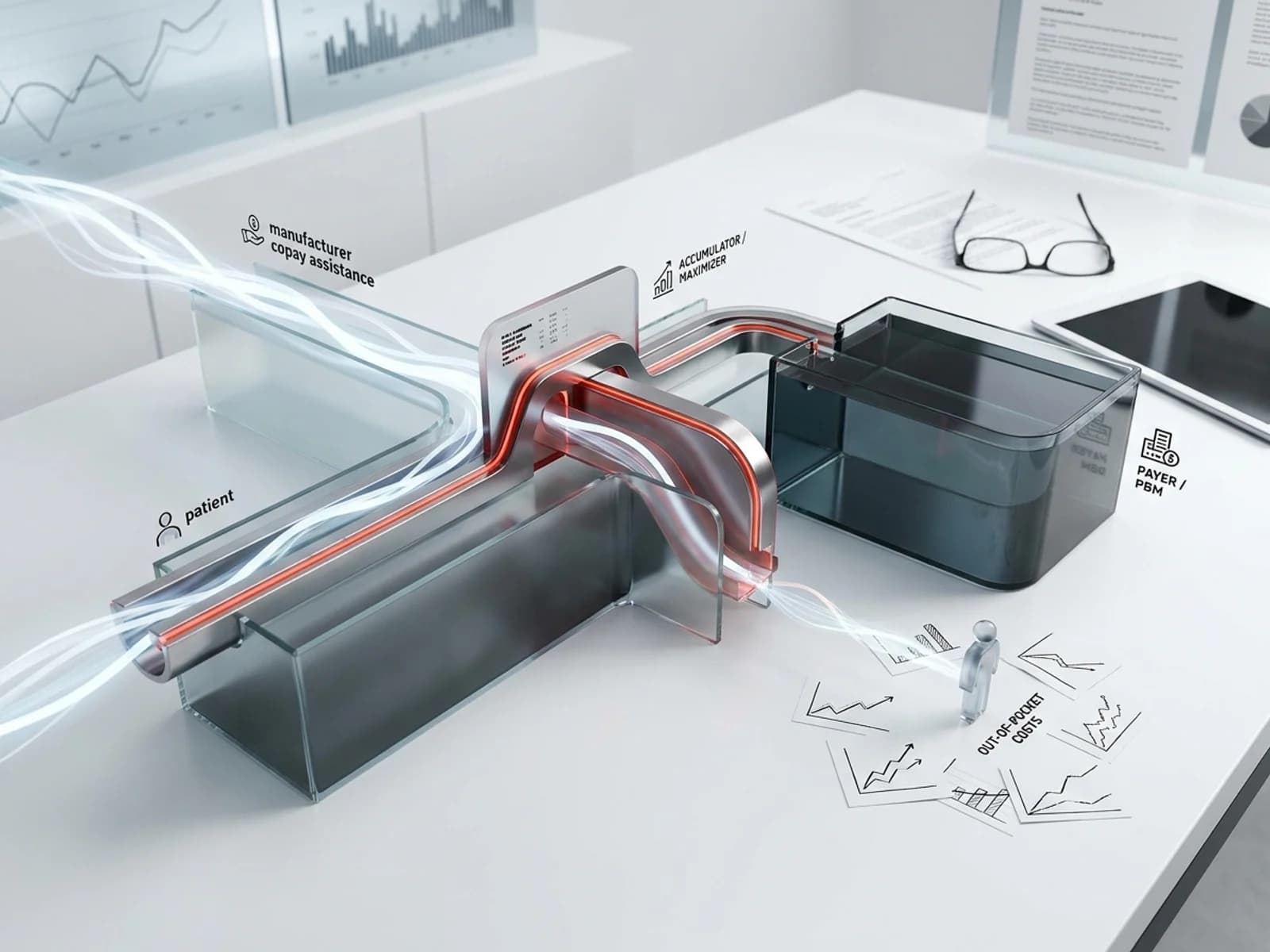
Copay accumulators, copay maximizers, and alternative funding programs each require different appeal strategies. The Triage Cancer 2026 Quick Guide defined the distinctions:
- Accumulators: Manufacturer copay assistance does not count toward deductible or out-of-pocket maximum. The patient faces the full cost-sharing obligation after the copay card is exhausted.
- Maximizers: The copay assistance is spread evenly across all fills in the plan year. The patient pays nothing during the year but does not progress toward their deductible or out-of-pocket maximum.
- Alternative funding programs (AFPs): The plan excludes selected specialty drugs from coverage and requires patients to apply for manufacturer patient assistance programs. If the patient does not qualify, the plan may deny coverage entirely.
Patients and provider teams must first determine which program is in effect, because the appeal arguments differ for each.
Step 1: Gather plan document evidence
Request the summary plan description and plan document
Under ERISA Section 104(b)(4), participants in ERISA-governed plans have the right to request plan documents, including the full plan document and summary plan description (SPD), within 30 days. The Wagner Law Group has noted that if plan documents do not describe appeal procedures, the participant may not be required to exhaust administrative remedies before filing suit.
For copay accumulator appeals, the plan document should specify:
- Whether the plan includes a copay accumulator, maximizer, or AFP provision
- How copay assistance is treated for cost-sharing purposes
- Whether the accumulator applies to all drugs or only to drugs with generic equivalents
- The plan's appeal procedures and timelines for benefit design challenges
Check for accumulator-specific disclosures
Some PBMs disclose accumulator programs in their formulary documentation or annual plan renewal materials. The Federal Register's January 2026 proposed rule on PBM fee disclosure noted that plans must provide detailed reports on net drug spending, rebates, and spread pricing, which may reveal accumulator configurations.
Key documents to request:
- Formulary documents: Check whether the drug is listed with accumulator notation
- Explanation of benefits (EOB): Look for accumulator-related codes or messages
- Annual enrollment materials: Some plans disclose accumulator programs during open enrollment
- PBM transparency reports: The 2026 federal PBM reform legislation requires semiannual reports to employer health plans
Identify whether the patient's plan is fully insured or self-funded
This determines which legal protections apply:
- Fully insured plans: Subject to state insurance regulations, including state accumulator bans. As of 2026, more than 25 states have laws restricting copay accumulator programs.
- Self-funded ERISA plans: Generally exempt from state insurance laws. State accumulator bans do not apply. Federal rules govern accumulator treatment.
- ACA Marketplace plans: Subject to federal cost-sharing rules. CMS's 2025 clarification established that all covered drugs in Marketplace plans are considered essential health benefits subject to annual cost-sharing limits.
Step 2: Determine applicable legal protections
State accumulator ban analysis
The NAIC working group reported that as of early 2026, 26 states plus DC and Puerto Rico have enacted laws restricting copay accumulator programs. But these laws vary in scope:
- Comprehensive bans: States like West Virginia prohibit accumulators in all cases, requiring all copay assistance to count toward patient cost-sharing limits.
- Generic-only restrictions: Eleven of the 26 state bans only prohibit accumulators when a generic equivalent is available. For specialty drugs without generic competition, accumulators remain legal.
- Maximizer gap: The JMCP primer on copay accumulators, copay maximizers, and alternative funding programs confirmed that no state law has yet directly addressed copay maximizer programs.
New Jersey's A.B. 5217, enacted January 2026, goes further than most state laws: it requires health plans to count any amount paid by or on behalf of the enrollee toward cost-sharing obligations and also prohibits copay maximizer programs and alternative funding programs. Each PBM operating in the state must annually certify compliance.
Federal regulatory status
The federal regulatory environment remains unsettled:
- 2021 CMS rule: Allowed health plans to use copay accumulator programs, deferring to state law.
- 2023 federal court decision: Struck down the CMS rule, barring insurers from implementing accumulators for drugs that lack generic equivalents.
- Current status: Plans can use accumulators for drugs with generic equivalents. For drugs without generic equivalents, the 2023 court decision creates ambiguity that has not been fully resolved by subsequent rulemaking.
- 2026 NBPP: The Departments of HHS, Labor, and Treasury stated their intent to issue future rulemakings on whether manufacturer assistance counts as cost-sharing under the ACA, but no final rule has been issued.
ERISA fiduciary duty arguments and emerging litigation
For self-funded ERISA plans, the appeal can argue that accumulator programs violate the plan fiduciary's duty of loyalty and prudence under ERISA Sections 404(a)(1)(A) and (B). The 2026 Newfront ERISA guide described the core fiduciary duties as "derived from trust law — described by courts as 'the highest duties known to the law.'"
Two recent class actions illustrate how ERISA fiduciary breach claims are being applied to copay accumulator programs. In Gluesing v. PrudentRx LLC & Caremark RX LLC (D.R.I., December 2024), the plaintiff alleged that the PBM and its affiliates breached ERISA fiduciary duties by failing to count prescription drug copays toward the plan participant's annual cost-sharing limitation, issuing wrongful pharmacy claim denials without proper notice, and instructing patients to obtain manufacturer assistance through misrepresentations. In Gurwitch v. Save on SP LLC (W.D.N.Y., January 2025), similar claims were brought under both ERISA and the Racketeer Influenced and Corrupt Organizations Act (RICO), alleging that copay assistance programs "deprive patients of the benefits of patient copay assistance funding and increase patients' healthcare costs."
Miller & Chevalier's ERISA litigation analysis noted that these cases assert PBM fiduciary status and challenge the legality of copay accumulator structures. While the outcomes remain pending, the litigation signals that patients and their counsel are increasingly using ERISA's fiduciary framework to challenge accumulator programs in court.
The argument is that by implementing an accumulator, the plan fiduciary is:
- Increasing patient out-of-pocket costs beyond what the plan document requires
- Diverting manufacturer assistance intended for patients to reduce plan liability
- Potentially discouraging medication adherence, which harms patient outcomes and may increase total plan costs
This argument is strongest when:
- The plan document does not explicitly authorize accumulator programs
- The accumulator creates a material increase in patient costs that was not disclosed during enrollment
- The patient can document that the accumulator caused therapy abandonment or nonadherence
Step 3: Structure the appeal
Internal appeal
The ERISA appeal process requires written submission within the plan's specified timeline — typically 180 days from the date of the adverse determination, though some plans allow only 60 days for health claims. The iLaw Digest 2026 ERISA appeals guide emphasized that the 180-day window starts when the patient receives the denial or accumulator notification, not when it is mailed.
For copay accumulator appeals, the internal appeal should include:
- Plan document citations: Quote the specific plan provisions that govern cost-sharing treatment, showing that the plan document either does not authorize accumulators or conflicts with the accumulator's operation.
- State law argument (for fully insured plans): Cite the applicable state accumulator ban and explain why the plan's accumulator violates state law.
- Federal court decision (for drugs without generic equivalents): Cite the 2023 federal court decision barring accumulators for drugs without generic equivalents.
- Clinical necessity statement: A letter from the prescriber explaining that the specialty drug is medically necessary, that there is no generic equivalent, and that the accumulator creates a risk of therapy interruption.
- Financial impact documentation: Evidence that the accumulator will cause the patient to face costs that exceed their ability to pay, creating a risk of abandonment.
External review
If the internal appeal is denied, patients in non-grandfathered plans can request external review by an independent review organization (IRO). The BCBS external review process guide for 2026 described external review as "the final escalation step when a plan denies a claim and internal appeals have failed."
For copay accumulator appeals, external review is available when:
- The denial involves medical judgment (e.g., the plan argues the drug is not medically necessary)
- The plan is subject to ACA external review requirements
- The patient files within four months of receiving the final internal appeal determination
The IRO's decision is binding on the plan. Patients must file within four months of the final internal denial.
ERISA litigation
If all administrative appeals are exhausted, patients can file suit in federal court under ERISA Section 502(a)(1)(B) to recover benefits due. The Springer Ayeni 2026 ERISA appeal guide noted that this requires exhaustion of all administrative remedies first.
Key considerations for ERISA litigation on accumulator issues:
- The administrative record is generally closed after appeal — new evidence cannot be introduced in court
- The standard of review depends on whether the plan grants the administrator discretionary authority
- Remedies are limited to recovery of benefits due; there is no jury trial and generally no damages beyond the benefit amount
When patient assistance still does not count
Generic-equivalent drugs
Under the current federal framework, plans can use accumulators for drugs with a generic equivalent. Even in states with broad accumulator bans, most laws do not prohibit accumulators when a generic equivalent is available. If the patient's specialty drug has an AB-rated generic, manufacturer copay assistance will not count toward cost-sharing regardless of the appeal.
Maximizers that spread assistance across the year
Maximizer programs technically provide the patient with zero out-of-pocket costs during the plan year, which makes them harder to challenge on financial-harm grounds. The patient's argument must focus on:
- The fact that the patient is not progressing toward their out-of-pocket maximum, creating risk if they switch drugs, switch plans, or lose copay card eligibility
- The plan document may not authorize the maximizer structure
- State laws may prohibit maximizers (New Jersey's A.B. 5217 is the most comprehensive example)
Alternative funding programs that exclude coverage
AFPs present the most severe access barrier because the drug is excluded from the plan formulary entirely. The PAN Foundation documented how AFPs work: "The health insurance plan excludes coverage for selected specialty medications, leaving you without coverage for these drugs under the plan benefits." The patient is redirected to apply for manufacturer PAPs, which have income eligibility criteria that may exclude middle-income patients.
Appealing AFP exclusions requires:
- Arguing that the plan's exclusion of a medically necessary drug violates the plan's coverage obligations
- Documenting that the patient does not qualify for the manufacturer PAP
- Challenging the AFP structure as a violation of ERISA fiduciary duties if the plan is self-funded
Sources
- The AIDS Institute, "Shortchanged: The Patient Impact of Copay Accumulator Policies in 2026." https://theaidsinstitute.org/media/documents/02-27-2026-09-23-55-TAI_2026_Report_final.pdf
- Triage Cancer, "Quick Guide to Co-pay Accumulators and Maximizers, 2026." https://triagecancer.org/wp-content/uploads/2026/03/2026-Quick-Guide-to-Co-pay-Accumulators-and-Maximizers-Alternative-Funding-Programs.pdf
- NAIC, "Prescription Drug Coverage (B) Working Group Materials." https://content.naic.org/sites/default/files/national_meeting/Materials%20-%20Prescription%20Drug%20Coverage%20%28B%29%20Working%20Group_1.pdf
- JMCP, "A Primer on Copay Accumulators, Copay Maximizers, and Alternative Funding Programs." https://pmc.ncbi.nlm.nih.gov/articles/PMC11293768
- ASHP, "Navigating Copay Adjustment Programs in Specialty Pharmacy." https://www.ashp.org/-/media/assets/specialty-pharmacy/docs/Navigating-Copay-Adjustment-Programs-in-Specialty-Pharmacy.pdf
- Federal Register, "Improving Transparency Into Pharmacy Benefit Manager Fee Disclosure (Proposed Rule, January 2026)." https://www.federalregister.gov/documents/2026/01/30/2026-01907/improving-transparency-into-pharmacy-benefit-manager-fee-disclosure
- Mintz, "PBM Policy and Legislative Update — Spring 2026." https://www.mintz.com/insights-center/viewpoints/2026-04-22-pbm-policy-and-legislative-update-spring-2026
- iLaw Digest, "Navigating the ERISA Appeals Process: A Step-by-Step Guide (2026 Edition)." https://ilawdigest.com/navigating-the-erisa-appeals-process-a-step-by-step-guide-2026-edition
- Muni Health, "BCBS External Review Process: How to Request Independent Medical Review 2026." https://muni.health/blog/bcbs-external-review-process-2026
- Springer Ayeni, "Understanding the ERISA Appeal Process." https://www.benefitslaw.com/articles/understanding-erisa-appeal-process
- Wagner Law Group, "Claims Appeals Procedures Must be in Formal Plan Documents." https://www.wagnerlawgroup.com/blog/2023/05/claims-appeals-procedures-must-be-in-formal-plan-documents
- PAN Foundation, "How Alternative Funding Programs Prevent Access to Medications." https://www.panfoundation.org/how-alternative-funding-programs-prevent-access-to-medications
- Immune Deficiency Foundation, "Addressing Copay Accumulators and Maximizers." https://primaryimmune.org/get-involved/advocate/addressing-copay-accumulators-and-maximizers
- HIV+Hepatitis Policy Institute, "Comments on the 2026 NBPP Proposed Rule." https://hivhep.org/wp-content/uploads/2024/11/HIV-Hep-2026-NBPP-Proposed-Rule-Comments-full-11.12.24.pdf
- 2026 Newfront ERISA for Employers Guide. https://go.newfront.com/hubfs/PDFs%20-%20Migrated/Newfront_ERISA_for_Employers_Guide.pdf
- Miller & Chevalier, "The ERISA Edit: PBMs Face ERISA Fiduciary Breach Claims in Two New Lawsuits." https://www.millerchevalier.com/publication/erisa-edit-pbms-face-erisa-fiduciary-breach-claims-two-new-lawsuits
- Federal Register, "Improving Transparency Into Pharmacy Benefit Manager Fee Disclosure (Proposed Rule, January 2026)." https://www.federalregister.gov/documents/2026/01/30/2026-01907/improving-transparency-into-pharmacy-benefit-manager-fee-disclosure
- NCBI/PMC, "A Primer on Copay Accumulators, Copay Maximizers, and Alternative Funding Programs." https://pmc.ncbi.nlm.nih.gov/articles/PMC11293768
- CMS, "Medicare Program; Contract Year 2027 Proposed Rule (April 2026)." https://www.federalregister.gov/documents/2026/04/06/2026-06600/medicare-program-contract-year-2027-and-certain-contract-year-2026-policy-and-technical-changes-to