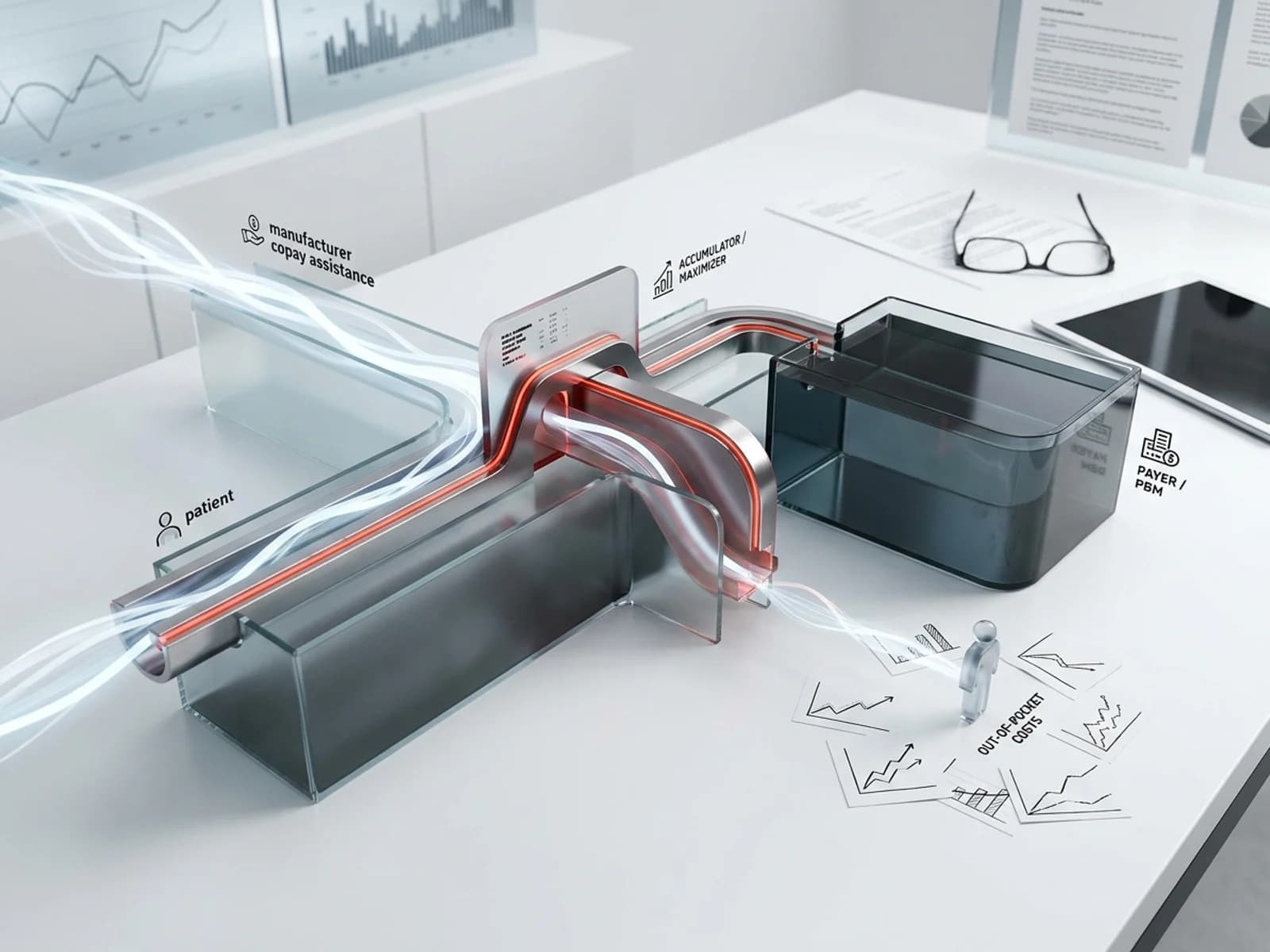
Manufacturer copay assistance programs exist to reduce out-of-pocket costs for patients taking specialty drugs. But since 2018, a parallel infrastructure of copay accumulator and maximizer programs has been redirecting those manufacturer funds. Instead of counting toward a patient's deductible and out-of-pocket maximum, copay assistance is intercepted by the plan or PBM and applied to the plan's cost. By September 2025, payers representing 84% of commercially insured lives had deployed at least one accumulator program, and 81% had deployed a maximizer program. IQVIA estimated that accumulators and maximizers consumed $4.8 billion in manufacturer copay assistance in 2023, more than double the 2019 figure.
This article is for manufacturer hub-services directors, patient-access program managers, market access leads, and commercial operations teams who need to monitor copay accumulator and maximizer activity, understand its impact on patient support program budgets, and respond strategically without undermining the programs that patients depend on.
How copay accumulators and maximizers work
The baseline: how copay assistance traditionally functions
When a manufacturer offers a copay assistance card for a specialty drug, the card reduces the patient's out-of-pocket cost at the pharmacy counter. Historically, the value of the card also counted toward the patient's annual deductible and out-of-pocket maximum under their commercial insurance plan. Once the patient met their out-of-pocket maximum, the plan covered the full cost of the drug for the remainder of the plan year. The manufacturer's copay assistance functioned as a bridge to the plan's cost-sharing protection.
Copay accumulator adjustment programs
Under a copay accumulator adjustment program, the manufacturer's copay assistance still reduces the patient's out-of-pocket cost at the point of sale, but the value of the assistance does not count toward the patient's deductible or annual out-of-pocket maximum. The manufacturer's funds pay for prescriptions until the annual copay card limit is reached. After that point, the patient is responsible for the full cost-sharing obligation from zero, because nothing has accumulated toward their deductible or out-of-pocket maximum.
The National Conference of State Legislatures describes the effect: "When the value of the coupon is exhausted at the pharmacy counter, the patient must then cover the full amount of his or her annual cost-sharing requirement until a deductible or out-of-pocket maximum is reached."
For a specialty drug costing $7,000 per fill with a $12,000 annual copay card limit and a patient deductible of $3,500, the accumulator works as follows:
| Fill | Patient pays | Copay card pays | Accumulated toward deductible |
|---|---|---|---|
| 1st | $0 | $7,000 | $0 |
| 2nd | $0 | $5,000 (card limit reached) | $0 |
| 3rd | $3,500 (deductible) | $0 | $3,500 |
| 4th+ | Copay/coinsurance | $0 | Continues to OOP max |
The patient faces a sudden, unanticipated cost at the third fill. According to IQVIA data cited by Rx Savings Solutions, this surprise copay scenario produces a 13x increase in discontinuation rates.
Copay maximizer programs
Copay maximizer programs take a different approach. Instead of letting the copay card run out and dumping costs on the patient, the maximizer spreads the manufacturer's copay assistance evenly across all fills in the plan year. The patient's cost share is set at a level that exactly exhausts the copay card's annual maximum over 12 months. The patient pays nothing out of pocket during the year, but the copay assistance never counts toward the deductible or out-of-pocket maximum.
For the same drug with a $12,000 copay card and 12 monthly fills at $7,000 each:
| Fill | Patient pays | Copay card pays | Accumulated toward OOP max |
|---|---|---|---|
| Each of 12 | $0 | $1,000 ($12,000 / 12) | $0 |
The patient pays nothing and may never realize that they are not progressing toward their out-of-pocket maximum. If they switch drugs mid-year, switch plans, or lose copay card eligibility, they face the full cost-sharing obligation from zero. The HIV+Hepatitis Policy Institute has documented maximizer scenarios where patients who were told their drug was "covered" faced sudden costs of $6,500 or more when their plan or drug changed.
Why payers use these programs
Payers and PBMs deploy accumulators and maximizers to reduce their own drug spending. By intercepting manufacturer copay assistance, the plan avoids paying the portion of the drug cost that would otherwise be covered after the patient meets their deductible or out-of-pocket maximum. The MMIT Network reported that payers target specialty drugs with significant manufacturer assistance and high budgetary impact. One payer stated that their PBM targets "any drug where a PAP is available."
The current landscape in numbers
Prevalence
According to MMIT's September 2025 survey:
- Accumulator programs: Payers representing 84% of commercial lives have implemented at least one accumulator program, up 3 percentage points from late 2023.
- Maximizer programs: Payers representing 81% of commercial lives have active maximizer programs, up 7 percentage points over two years.
- Both figures are expected to remain stable, as payers who have not yet implemented these programs cite regulatory constraints, administrative complexity, and member disruption as barriers.
The KFF reported that a 2023 survey of 35 PBMs and payers representing nearly 118 million commercially insured individuals found that 49% of those enrollees were in a plan with a copay maximizer program, an approximately eight-fold increase since 2018. MMIT's more recent survey found that by Q3 2025, payers anticipated 46% of plan sponsors would opt into an accumulator program and 53% into a maximizer program, with member enrollment projected to reach 48% for accumulators and 57% for maximizers by fall 2025.
Financial scale
IQVIA estimated that copay accumulator and maximizer programs accounted for $4.8 billion in manufacturer copay assistance in 2023, more than double the $2.2 billion attributed to these programs in 2019. This figure represents manufacturer funds that were diverted from their intended purpose of reducing patient out-of-pocket costs and instead offset plan liabilities.
State legislative response
As of 2025, 25 states, the District of Columbia, and Puerto Rico have enacted laws restricting copay accumulator programs in state-regulated health plans. Avalere Health's analysis of AIS Health Data's September 2025 enrollment data found that at least 16.8% of the total U.S. commercial market (approximately 34.28 million individuals) are enrolled in plans that must count copay assistance toward patient cost-sharing limits.
But these laws have significant limitations:
- ERISA preemption: State insurance laws do not apply to self-funded employer plans governed by the Employee Retirement Income Security Act (ERISA). Self-funded plans cover approximately 63% of covered workers at private firms nationally. A LinkedIn post by Adam Fein noted that even in Connecticut, which has banned accumulators, the state government's own employee plan uses an accumulator.
- Generic-only restrictions: Eleven of the 25 state bans only prohibit accumulators when a generic equivalent is available. For specialty drugs without generic competition, accumulators remain legal even in these states.
- Maximizer gap: No state law has yet directly addressed copay maximizer programs. The NCSL confirmed this gap in its 2025 overview of copayment adjustment programs.
Federal regulatory status
The federal regulatory environment remains unsettled:
- In 2021, CMS allowed health plans to use copay accumulator programs, deferring to state law. In 2023, a federal court struck down this rule, barring insurers from implementing accumulators for drugs that lack generic equivalents.
- CMS's 2025 rules clarified that in ACA Marketplace plans, all covered drugs are considered essential health benefits (EHBs) and are subject to annual cost-sharing limits.
- The 2026 proposed Notice of Benefit and Payment Parameters (NBPP) did not expand these protections. Instead, the Departments of HHS, Labor, and Treasury stated their intent to issue two future rulemakings: one to extend EHB protections to employer-sponsored and self-insured plans, and another to clarify whether manufacturer assistance counts as "cost-sharing" under the ACA.
- Patients Rising reported that until those future rules are finalized, plans can continue using accumulators and maximizers.
What manufacturer support teams should monitor
Tracking which plans are running accumulators versus maximizers
Manufacturer hub teams should maintain a real-time map of which major commercial plans and PBMs are deploying accumulators, maximizers, or both, and for which therapeutic areas. Key data sources include:
- Payer and PBM transparency reports: Some PBMs disclose accumulator and maximizer programs in their formulary documentation.
- Hub call-center data: Patient calls reporting unexpected out-of-pocket costs, rejected copay cards, or changed cost-sharing amounts are an early signal that a plan has initiated or changed its accumulator/maximizer configuration.
- Specialty pharmacy feedback: Because most accumulators and maximizers require prescriptions to be routed through the payer's preferred specialty pharmacy (handling an average of 68% of total specialty claims, per MMIT), specialty pharmacy partners can identify when a patient's claim is being processed under an accumulator or maximizer protocol.
- Third-party tracking services: Several market access analytics firms track accumulator and maximizer deployment by plan, PBM, and drug.
Monitoring copay card exhaustion rates
The most direct signal of accumulator activity is a spike in copay card exhaustion. In a standard benefit design, copay assistance counts toward the deductible and out-of-pocket maximum, so the card's annual value is consumed over the first few fills and then the plan's cost-sharing protection takes over. Under an accumulator, the card's value is consumed at the same rate, but the patient's cost-sharing obligation is untouched.
Support teams should track:
- Exhaustion timing: How many months into the plan year are copay cards running out? A shift from month 3–4 to month 2–3 suggests increasing accumulator penetration.
- Abandonment rates after exhaustion: Patients who face the full cost-sharing obligation mid-year may abandon therapy. A spike in discontinuation at a predictable point in the plan year is an accumulator signature.
- Geographic patterns: State-level accumulator bans create a patchwork. Abandonment rates should be lower in states with broad accumulator bans (e.g., West Virginia, which bans accumulators in all cases) than in states with no restrictions.
Tracking patient cost exposure
Under maximizer programs, patients may not experience any out-of-pocket costs during the plan year, but they are not progressing toward their deductible or out-of-pocket maximum. If the patient changes drugs, changes plans, or loses copay card eligibility, they face the full cost-sharing obligation from zero. Manufacturer teams should monitor:
- Mid-year therapy switches: Patients switching from a maximizer-managed drug to a different drug mid-year may face the full annual cost-sharing obligation on the new drug because nothing accumulated on the prior drug.
- Plan-year transitions: Patients moving from one plan year to the next may discover that their copay card no longer covers the redesigned cost-sharing structure.
- Copay card eligibility changes: If a manufacturer modifies copay card terms (annual maximum, income eligibility), patients in maximizer programs may face unexpected costs because the maximizer was calibrated to the old card value.
Monitoring the shift from accumulators to maximizers to alternative funding programs
Drug Channels Institute has documented a progressive shift from accumulators to maximizers and, more recently, to alternative funding programs (AFPs). AFPs go further than maximizers: they identify patients on high-cost specialty drugs, exclude those drugs from the plan formulary, and require patients to apply for manufacturer patient assistance programs (PAPs) or free-drug programs instead. If the patient qualifies, the drug is provided at no cost to the plan. If the patient does not qualify, the plan may deny coverage entirely.
Shawn Gremminger, quoted on LinkedIn, described the progression as "a bad soap opera" where "accumulators are easily defensible on fairness grounds. Maximizers less so. And AFPs are borderline fraudulent."
Manufacturer teams should watch for:
- Plans moving from accumulator-only to accumulator-plus-maximizer configurations
- Plans or PBMs partnering with AFP vendors (such as ProgramData, AffordRx, or similar entities)
- Specialty pharmacy exclusivity requirements that concentrate claims in payer-controlled channels
Strategic responses
Structuring copay programs to minimize diversion
Several structural approaches can reduce the effectiveness of accumulators and maximizers:
- Income-verified programs: Programs that verify patient income and adjust assistance based on financial need may qualify for different regulatory treatment than open copay cards. Some state accumulator bans exempt income-verified assistance.
- Patient-pay-first designs: Programs that require the patient to pay a minimum amount before assistance kicks in may reduce the amount of funds available for interception by the plan.
- Split-funding models: Dividing assistance between copay cards and direct patient support (such as nurse support, adherence programs, or injection training) moves funds away from the pharmacy claim transaction where accumulators and maximizers operate.
Advocacy and legislative engagement
Manufacturers have engaged in state legislative advocacy to expand accumulator bans. Industry trade groups including BIO and PhRMA have supported state-level legislation. Key advocacy positions include:
- Expanding state bans to cover maximizer programs, not just accumulators
- Closing the generic-only loophole in states that restrict accumulators only when a generic is available
- Supporting federal rulemaking to classify manufacturer copay assistance as cost-sharing under the ACA
- Opposing alternative funding programs that exclude drugs from formulary coverage
Data-driven program design
Support teams should use accumulator and maximizer prevalence data to model copay program budgets. If 84% of commercial lives face accumulator exposure, the expected budget consumption per patient is materially higher than in a traditional benefit design. Key modeling inputs:
- Percentage of patients in self-funded ERISA plans (not protected by state bans)
- Therapeutic area competition: drugs with generic equivalents face different accumulator dynamics than sole-source specialty drugs
- Plan year timing: January 1 plan-year starts create predictable exhaustion patterns
- Copay card annual maximum relative to the patient's annual cost-sharing obligation
Key regulatory and data sources
| Source | Reference |
|---|---|
| NCSL, Copayment Adjustment Programs (2025) | https://www.ncsl.org/health/copayment-adjustment-programs |
| KFF, Copay Adjustment Programs (2025) | https://www.kff.org/health-costs/copay-adjustment-programs-what-are-they-and-what-do-they-mean-for-consumers |
| MMIT, Inside the Payer Playbook: Copay Accumulators and Maximizers (Dec 2025) | https://www.mmitnetwork.com/thought-leadership/inside-payer-playbook-copay-accumulators-maximizers-part-1 |
| MMIT, Implications for Pharma (Dec 2025) | https://www.mmitnetwork.com/thought-leadership/copay-accumulators-maximizers-part-2-implications-pharma |
| Avalere Health, State Copay Accumulator Bans (2025) | https://advisory.avalerehealth.com/insights/state-copay-accumulator-bans-now-affect-at-least-17-of-commercial-lives |
| HIV+Hepatitis Policy Institute, NBPP Comments (2026) | https://hivhep.org/testimony-comments-letters/comments-on-the-2026-nbpp-proposed-rule |
Sources
- NCSL, "Copayment Adjustment Programs." https://www.ncsl.org/health/copayment-adjustment-programs.
- CMS, Notice of Benefit and Payment Parameters for 2021 Final Rule. https://www.federalregister.gov/documents/2020/05/14/2020-10142/patient-protection-and-affordable-care-act-hhs-notice-of-benefit-and-payment-parameters-for-2021.
- CMS, Notice of Benefit and Payment Parameters for 2024 Final Rule. https://www.federalregister.gov/documents/2023/04/28/2023-08515/patient-protection-and-affordable-care-act-improving-health-and-affordability-of-insurance.
- KFF, "Copay Adjustment Programs: What Are They and What Do They Mean for Consumers?" https://www.kff.org/health-costs/copay-adjustment-programs-what-are-they-and-what-do-they-mean-for-consumers.
- MMIT, "Inside the Payer Playbook: Copay Accumulators and Maximizers, Part 1," December 2025. https://www.mmitnetwork.com/thought-leadership/inside-payer-playbook-copay-accumulators-maximizers-part-1.
- MMIT, "Copay Accumulators and Maximizers, Part 2: Implications for Pharma," December 2025. https://www.mmitnetwork.com/thought-leadership/copay-accumulators-maximizers-part-2-implications-pharma.
- Avalere Health, "State Copay Accumulator Bans Now Affect At Least 17% of Commercial Lives." https://advisory.avalerehealth.com/insights/state-copay-accumulator-bans-now-affect-at-least-17-of-commercial-lives.
- HIV+Hepatitis Policy Institute, "Comments on the 2026 NBPP Proposed Rule." https://hivhep.org/testimony-comments-letters/comments-on-the-2026-nbpp-proposed-rule.
- HIV+Hepatitis Policy Institute, "Policy Updates: Copay Accumulators, Maximizers, AFPs and Beyond," November 2024. https://hivhep.org/wp-content/uploads/2024/11/Policy-Updates-Copay-Accumulators-Maximizers-AFPs-and-Beyond-11.18.24.pdf.
- JMCP, "A primer on copay accumulators, copay maximizers, and alternative funding programs." https://www.jmcp.org/doi/10.18553/jmcp.2024.30.8.883.
- Patients Rising, "Copay Help Tricks: Why Insurance May Block Your Med Savings." https://www.patientsrising.org/advocacy-updates/copay-accumulators-maximizers-nbpp-2026-what-patients-need-to-know.
- JHOP, "Copay Maximizer Programs Replacing Accumulator Programs with Ramifications for Patient Out-of-Pocket Expenses," April 2026. https://www.jhoponline.com/web-exclusives/copay-maximizer-programs-replacing-accumulator-programs-with-ramifications-for-patient-out-of-pocket-expenses.
- Drug Channels Institute, "Copay Accumulators and Maximizers in 2025: Popular, Profitable, and Problematic," February 2026. https://www.drugchannels.net/2026/02/copay-accumulators-and-maximizers-in.html.
- Rx Savings Solutions, "All About Specialty Copay Programs." https://rxss.com/blog/specialty-copay-programs-accumulate-maximize-or-avoid.
- PAN Foundation, "Protecting Your Access to Medications." https://www.panfoundation.org/protecting-your-access-to-medications.
- California Health Benefits Review Program, "SB 1199 Prescription Drug Cost Sharing Technical Brief." https://www.chbrp.org/sites/default/files/bill-documents/SB1199/SB%201199%20Prescription%20Drug%20Cost%20Sharing%20Report%20-%20Tech_Brief_Final.pdf.