On April 14, 2026, CMS published the proposed rule "Interoperability Standards and Prior Authorization for Drugs" (CMS-0062-P) in the Federal Register. For the first time, the rule would extend electronic prior authorization requirements to prescription drugs, including specialty drugs billed under the medical benefit. If finalized as proposed, most requirements take effect October 1, 2027—giving manufacturers, hub teams, specialty pharmacies, and access technology vendors roughly 18 months from the proposal date to prepare.
This article explains what CMS-0062-P requires for drug prior authorization, where specialty-drug workflows are least prepared, and what manufacturer market access teams, hub operators, and specialty pharmacy technology teams should do before the compliance date.
It is written for manufacturer market access and hub teams, specialty pharmacy operations staff, payer strategy teams, and health technology vendors who build or support prior authorization workflows for specialty drugs.
What CMS-0062-P proposes
CMS-0062-P builds on two earlier rules: the 2020 CMS Interoperability and Patient Access final rule (CMS-9115-F) and the 2024 CMS Interoperability and Prior Authorization final rule (CMS-0057-F). The 2024 rule required electronic prior authorization for non-drug items and services beginning January 1, 2027. CMS-0062-P closes the drug gap.
Key requirements
| Requirement | What it means | Compliance date |
|---|---|---|
| Medical-benefit drug PA through Prior Authorization API | Impacted payers must incorporate drug coverage and documentation requirements into the existing FHIR-based Prior Authorization API | October 1, 2027 |
| Pharmacy-benefit drug PA through NCPDP standards | Medicaid FFS, Medicaid managed care, CHIP, and QHP issuers on FFEs must support SCRIPT, Formulary & Benefit, and Real-Time Prescription Benefit (RTPB) standards for pharmacy-benefit drug PA | October 1, 2027 |
| Drug PA decision timeframes | 24 hours for outpatient drugs (Medicaid/CHIP); 72 hours standard / 24 hours expedited for QHPs | October 1, 2027 |
| Specific denial reason required | Payers must provide a specific reason for denying any drug PA request | October 1, 2027 |
| Drug PA metrics reporting | Impacted payers must publicly report drug PA metrics beginning in 2028 (for the 2027 reporting period) | 2028 |
| FHIR endpoint registry | Impacted payers must publish FHIR API endpoints directly to CMS | October 1, 2027 |
Which payers are impacted
The rule applies to Medicare Advantage organizations, state Medicaid and CHIP fee-for-service programs, Medicaid managed care plans, CHIP managed care entities, and Qualified Health Plan issuers on the Federally Facilitated Exchanges (FFE)—including a new requirement for small-group market QHP issuers on the FF-SHOPs.
Which drugs are covered
All drugs. The rule explicitly covers specialty drugs administered under the medical benefit (buy-and-bill biologics, infused therapies, physician-administered oncology agents) through the FHIR-based Prior Authorization API, and drugs dispensed through the pharmacy benefit through NCPDP standards. CMS states that "FHIR and NCPDP standards are mutually exclusive and, when used in conjunction, encompass the full scope of drugs that are covered by any particular payer."
Where specialty-drug PA workflows are least prepared
Medical-benefit drug PA is the biggest gap
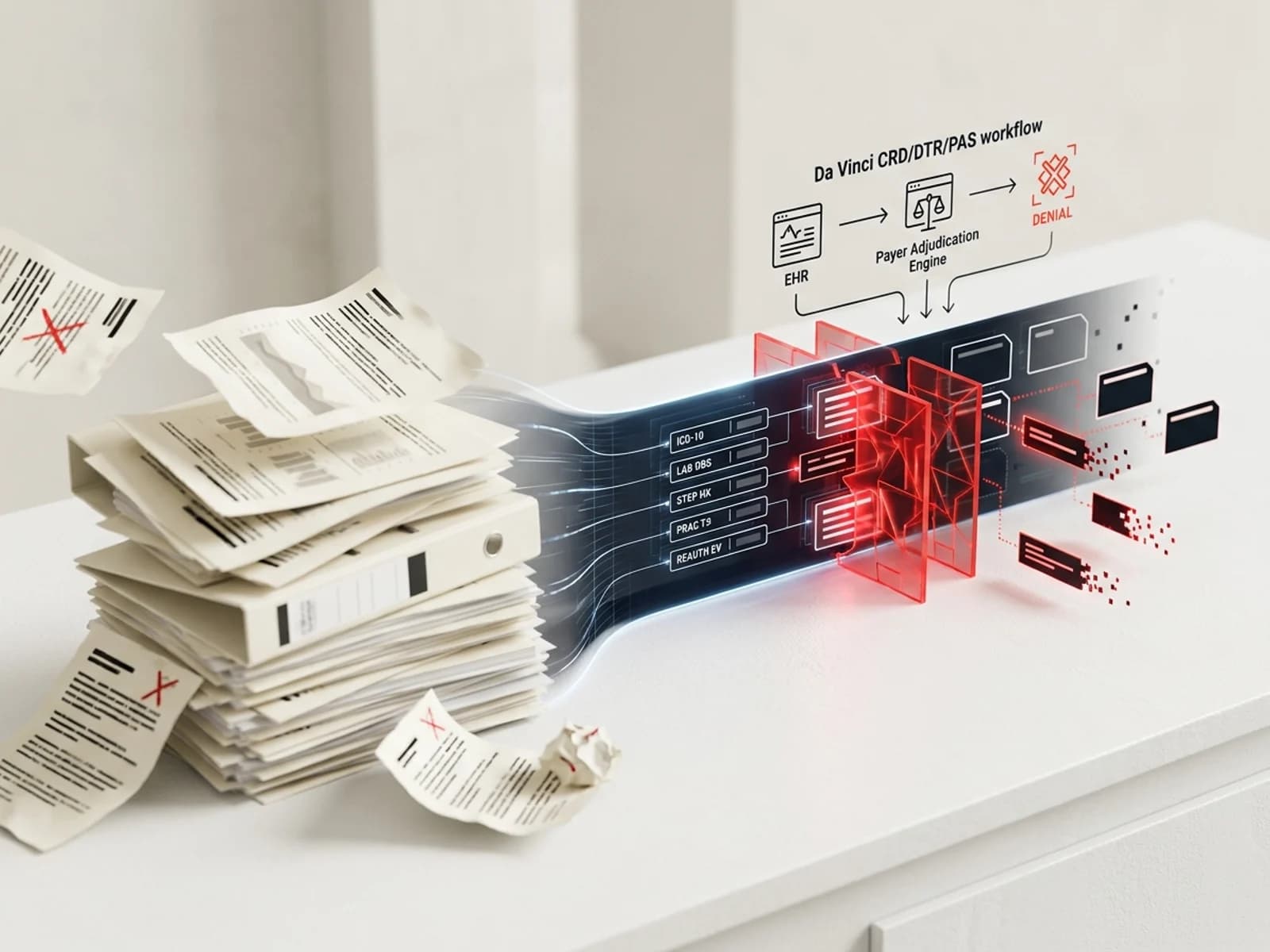
The 2024 rule (CMS-0057-F) required electronic PA for non-drug items and services. Most payers have implemented or are implementing FHIR-based Prior Authorization APIs for procedures, devices, and services. But drug PA—particularly for specialty drugs billed under the medical benefit—remains largely manual. A 2026 analysis by the American Osteopathic Association noted that specialty-drug PA is "one of the most significant sources of administrative burdens in healthcare."
Medical-benefit drug PA today relies on fax, phone, payer portals, and electronic form platforms like CoverMyMeds. CMS acknowledges this gap: the proposed rule states that "incorporating drugs into Prior Authorization APIs means that information is available through the API as to whether prior authorization is required for drugs covered under a medical benefit, the coverage and documentation requirements for prior authorization are available, and that the API can transmit prior authorization requests and decisions between providers and the payer."
For specialty drugs, the gap is acute because:
- Documentation requirements are complex: Medical-benefit specialty drug PA typically requires diagnosis codes, lab values, biomarker test results, treatment history, step therapy documentation, prescriber specialty verification, and imaging results. These data live across multiple EHR modules and are rarely structured in a way that maps cleanly to FHIR resources.
- The buy-and-bill workflow is different: Physician-administered drugs go through J-code billing under Medicare Part B or medical benefit under commercial plans. The PA submission, approval, and claims submission are separate workflows that often involve different departments within the same payer.
- Reauthorization is frequent: Specialty drug PA often requires reauthorization every 3–12 months. The FHIR-based workflow must support renewal submissions with updated clinical data, not just initial authorization.
Pharmacy-benefit specialty drug PA is closer to ready
Pharmacy-benefit PA for specialty drugs already uses some electronic standards. Medicare Part D sponsors are required to support ePA through NCPDP SCRIPT, and most PBMs have implemented some level of electronic PA for pharmacy-benefit drugs. CMS-0062-P extends these requirements to Medicaid FFS, Medicaid managed care, CHIP, and QHP issuers—which have farther to go.
The three NCPDP standards required are:
- SCRIPT: Supports electronic PA request and response for pharmacy-benefit drugs
- Formulary & Benefit (F&B): Allows providers to query formulary information including PA requirements
- Real-Time Prescription Benefit Check (RTPB): Allows real-time coverage and cost verification at the point of prescribing
Implementation guides and technical standards
CMS proposes requiring impacted payers to conform to specific FHIR implementation guides (IGs):
| Implementation guide | Version | Function |
|---|---|---|
| Da Vinci PAS (Prior Authorization Support) | 2.2.1 | Medical-benefit drug PA request and response |
| Da Vinci CRD (Coverage Requirements Discovery) | 2.2.1 | Query whether PA is required and what documentation is needed |
| Da Vinci DTR (Documentation Templates and Rules) | 2.2.0 | Generate and complete PA documentation templates |
| CARIN Blue Button | 2.2.0 | Patient access to PA status and decisions |
| Da Vinci PDex (Payer Data Exchange) | 2.1.0 | Payer-to-Payer data exchange including PA history |
CMS also proposes that older STU 2-era IG versions expire January 1, 2028—meaning payers and providers must be on the current versions by that date.
The FHIR vs NCPDP split
A key architectural decision in the rule: FHIR handles medical-benefit drug PA, NCPDP handles pharmacy-benefit drug PA. For specialty drugs that can be billed under either benefit (e.g., subcutaneous biologics, oral oncolytics), the pathway depends on how the specific plan processes the claim. This means:
- Manufacturer hub teams need to determine which benefit pathway applies during benefits investigation
- Technology vendors need to support both FHIR-based and NCPDP-based PA workflows
- Payer systems need to maintain both pathways and ensure they return consistent coverage determinations
What manufacturer and hub teams should fix now
1. Audit your current PA submission channels
Map every PA submission pathway your hub uses today—for every product, every payer type, and every benefit pathway. For each, document:
- Current submission method (fax, portal, CoverMyMeds, Surescripts, direct API)
- Whether it supports electronic clinical documentation attachment
- Whether it can receive structured denial reasons
- Average turnaround time and denial rate by channel
This audit reveals which pathways will need the most rework to comply with the 2027 deadline.
2. Prepare structured clinical data payloads
FHIR-based PA requires structured clinical data. Today, most specialty drug PA relies on unstructured documents—PDFs, chart notes, narrative letters of medical necessity. The transition to FHIR means that diagnosis, labs, biomarker results, treatment history, and prescriber information will need to travel as coded data elements.
Manufacturer hub teams should:
- Work with their technology vendors to map current PA documentation to FHIR clinical resources (Condition, Observation, MedicationRequest, DiagnosticReport)
- Build data validation that checks PA submissions for completeness before they reach the payer
- Test with early-adopter payers who have already implemented the PAS IG
3. Prepare for 24-hour decision timeframes
CMS proposes a 24-hour decision timeframe for outpatient drug PA requests under Medicaid and CHIP. For QHP issuers, the proposed timeframes are 72 hours (standard) and 24 hours (expedited). These are significantly faster than current practice for many specialty drugs.
This compressed timeline affects:
- Hub case management: Cases that currently take 3–5 days to resolve may need to be decided within 24 hours of submission
- Peer-to-peer scheduling: If a denial is issued, the appeal or peer-to-peer must happen faster
- Manufacturer bridge supply: Shorter decision windows may reduce the need for bridge programs, but access teams should verify this during benefits investigation
4. Build denial-reason analytics
CMS-0062-P requires payers to provide specific denial reasons for drug PA requests. This is a significant transparency improvement. Today, denial reasons are often vague or buried in portal workflows. The new requirement means:
- Every denial must include a machine-readable reason code
- Denials must include the specific documentation gap or clinical criterion not met
- This data should feed directly into manufacturer PA denial analytics
Manufacturer access teams should build reporting infrastructure that captures structured denial reasons and maps them to clinical documentation gaps. This data drives hub training, field reimbursement education, and payer strategy.
5. Engage with the FHIR ecosystem
CMS has established an Electronic Prior Authorization Acceleration initiative with early adopters including health systems, EHR vendors, and payers. CMS Administrator Dr. Mehmet Oz described prior authorization as an issue that requires the entire healthcare system — payers, providers, and technology vendors — to work together on shared standards and real-world workflow fixes, not technology alone.
Manufacturer teams should:
- Participate in Da Vinci implementation guide connectathons and testing events
- Engage with their EHR vendor partners on PAS IG readiness
- Join CMS-sponsored testing opportunities ahead of the 2027 compliance date
- Submit comments on CMS-0062-P by the June 15, 2026 deadline, particularly on specialty-drug-specific concerns: documentation requirements, reauthorization workflows, and the interaction between FHIR-based medical benefit PA and NCPDP-based pharmacy benefit PA
What specialty pharmacy teams should do
Specialty pharmacies that handle pharmacy-benefit PA should:
- Verify NCPDP SCRIPT readiness: Confirm that your dispensing system supports SCRIPT ePA for all required payer types, not just Medicare Part D
- Map F&B data flow: Ensure formulary and benefit queries return accurate PA requirements for specialty drugs across all contracted payers
- Build RTPB integration: Real-time prescription benefit checks should return specialty drug coverage, copay, and PA requirements at the point of prescribing
Specialty pharmacies that handle medical-benefit drugs (buy-and-bill, REMS-restricted products) should:
- Understand the FHIR PA workflow: Medical-benefit drug PA will use the same Prior Authorization API as procedures and services, but with drug-specific documentation templates
- Prepare for structured clinical data exchange: The DTR IG will generate documentation templates based on payer coverage requirements; specialty pharmacy staff will need to populate these with structured data
- Coordinate with provider offices: Most medical-benefit PA is still initiated by the prescriber's office; specialty pharmacies should offer to support the electronic submission process
What the rule does not address
CMS-0062-P leaves several specialty-drug PA issues unresolved:
- Step therapy verification: CMS requests comment on whether payers should honor step therapy completion from prior payers via the Payer-to-Payer API, but does not propose requiring it
- Off-label use documentation: The rule does not specify how off-label or compendia-supported use should be documented in the FHIR workflow
- Biomarker and diagnostic test integration: The rule does not address how companion diagnostic results should flow through the PA API
- Multi-indication PA: Drugs approved for multiple indications may have different PA criteria for each; the rule does not specify how indication-specific documentation should be structured
These gaps may be addressed in the final rule or subsequent guidance, and manufacturer teams should monitor CMS rulemaking and Da Vinci IG updates.
Timeline: what to do when
| Timeframe | Action |
|---|---|
| Now through June 15, 2026 | Submit comments on CMS-0062-P; begin PA channel audit |
| Q3–Q4 2026 | Map documentation to FHIR resources; engage EHR vendors on PAS IG testing |
| Q1 2027 | Begin testing with early-adopter payers; train hub staff on structured PA submission |
| Q2–Q3 2027 | Full testing with all contracted payers; update denial analytics for structured reasons |
| October 1, 2027 | Compliance date: medical-benefit drug PA through Prior Authorization API, pharmacy-benefit drug PA through NCPDP standards |
| January 1, 2028 | Older IG versions expire; all systems must be on current versions |
| 2028 | First drug PA metrics reporting period (reporting 2027 data) |
What to monitor
- CMS-0062-P final rule: CMS accepted comments through June 15, 2026. The final rule may adjust compliance dates, scope, or technical standards
- Da Vinci IG updates: PAS, CRD, and DTR IGs are updated regularly; manufacturers should track version changes
- Payer readiness: CMS has announced early adopters in its ePA Acceleration initiative; monitor which payers go live with drug PA APIs first
- State Medicaid readiness: State Medicaid FFS programs and managed care plans have varying levels of ePA infrastructure; the October 2027 deadline will require significant upgrades in some states
- NCPDP standard updates: SCRIPT, F&B, and RTPB standards are maintained by NCPDP; monitor for version changes that could affect pharmacy-benefit PA workflows
This article is for informational purposes only and does not constitute legal advice, regulatory compliance guidance, or reimbursement guidance for any specific entity. CMS-0062-P is a proposed rule and its requirements may change before finalization. Always consult the final rule and applicable CMS guidance for compliance obligations.
Last updated: May 31, 2026.
Sources
- CMS. "2026 CMS Interoperability Standards and Prior Authorization for Drugs Proposed Rule (CMS-0062-P)." April 14, 2026. cms.gov
- Federal Register. "Medicare and Medicaid Programs: Interoperability Standards and Prior Authorization for Drugs." 91 FR 19891. April 14, 2026. federalregister.gov
- CMS. "Electronic Prior Authorization Overview." 2026. cms.gov
- CMS. "CMS-0062-P Briefing Slides." April 2026. cms.gov
- CMS. "CMS-0062-P Comment Guide." May 2026. cms.gov
- Crowell & Moring. "CMS Seeks to Expand Interoperability Requirements to Drug Pre-Authorization: FAQ." April 29, 2026. crowell.com
- American Osteopathic Association. "New CMS proposed rule expands electronic prior authorization requirements to prescription drugs." May 5, 2026. osteopathic.org
- AHIMA. "CMS Interoperability Standards and Prior Authorization for Drugs Proposed Rule Fact Sheet." 2026. ahima.org
- Onyx Health. "CMS-0062: What Payers Need to Know." 2026. onyxhealth.io
- Frier Levitt. "CMS Proposed Rule on Electronic Prior Authorization for Drugs: Key Impacts and Comment Deadline." 2026. frierlevitt.com
- CMS. "CMS Announces Early Adopters to Advance Solutions for Electronic Prior Authorization." 2026. cms.gov
- American College of Cardiology. "CMS Releases 2027 IPPS, Interoperability and Prior Auth Proposed Rules." April 16, 2026. acc.org