Under CMS-0057-F, impacted payers must implement FHIR-based Prior Authorization APIs by January 1, 2027. The CMS-0062-P proposed rule, published April 14, 2026, would extend those requirements to all drugs—including specialty drugs under the medical benefit—by October 1, 2027. When prior authorization moves from faxed narrative letters to structured FHIR resources, the failure modes change. A payer's automated adjudication engine no longer reads clinical notes; it evaluates coded fields in Claim.supportingInformation, Condition resources, and ServiceRequest payloads. If a required field is missing, truncated, or coded at the wrong specificity, the request dies in the payer's rules engine before a nurse or medical director ever sees it.
This article is for manufacturer market access teams, hub operators, specialty pharmacy technology staff, and provider-facing reimbursement specialists who need to understand which FHIR data fields cause automated specialty-drug PA denials and what to fix before the API deadline makes these failures systemic.
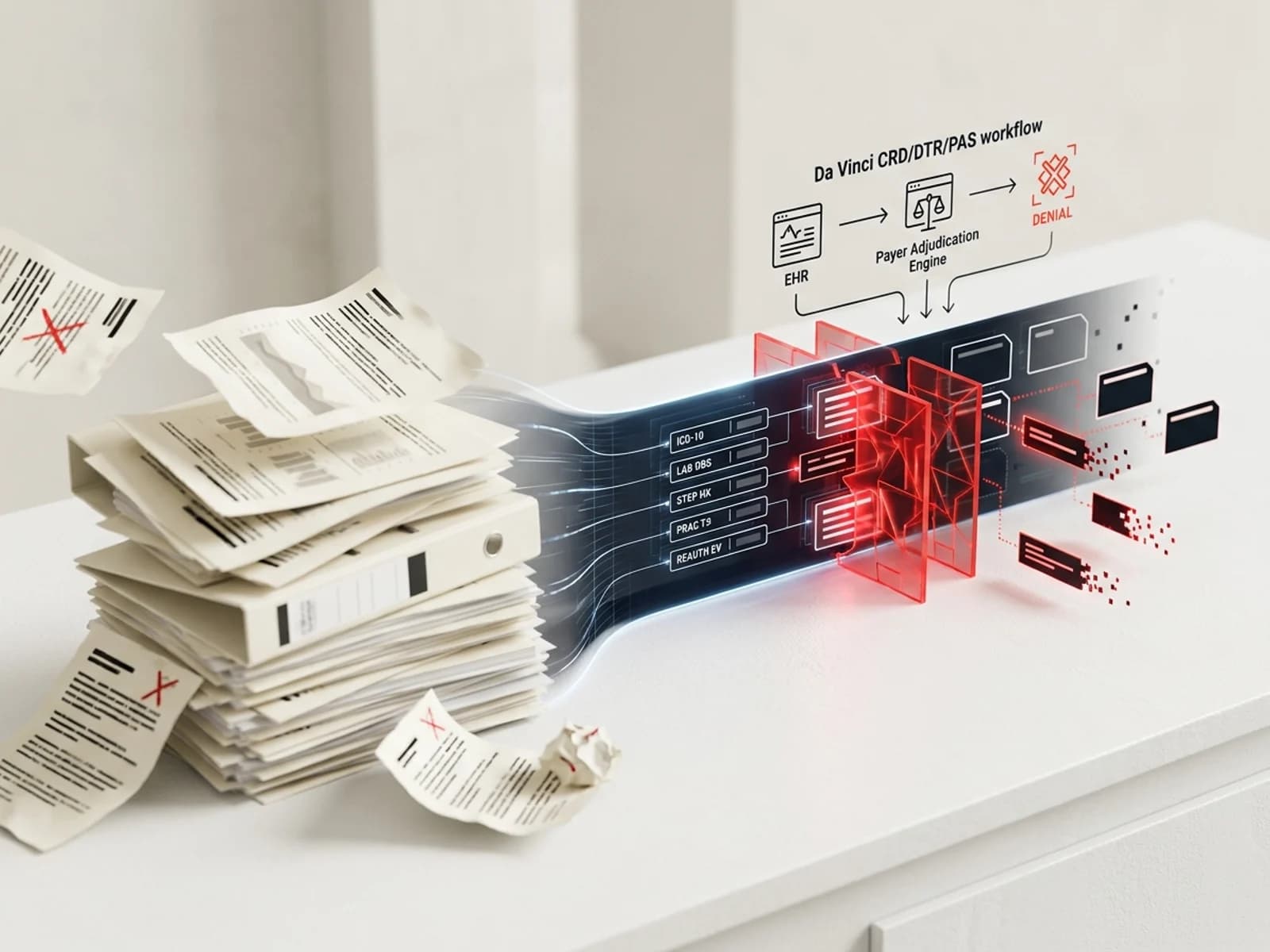
How FHIR-based prior authorization works
The HL7 Da Vinci project defines three implementation guides that together form the electronic prior authorization workflow:
Coverage Requirements Discovery (CRD) — At order entry, the EHR sends a CDS Hooks request to the payer. The payer returns whether PA is needed and what documentation the plan requires.
Documentation Templates and Rules (DTR) — The payer returns a FHIR Questionnaire specifying the clinical evidence required: diagnosis codes, lab values, imaging results, prior treatment history, prescriber credentials, and outcome measures. The DTR engine pulls answers from the EHR where available.
Prior Authorization Support (PAS) — The provider submits a FHIR
Claimresource withsupportingInformationcontaining the completed documentation. The payer returns aClaimResponsewith per-item decisions.
Each stage depends on structured, coded data. If the EHR cannot populate a field, or if the field is populated with a code the payer's rules engine does not recognize, the result is an automated denial.
Five FHIR fields that cause the most specialty-drug denials
1. Diagnosis code specificity (Condition.code → ICD-10-CM)
What happens: The PAS Claim resource includes diagnosis references through Claim.diagnosis elements, which point to Condition resources. Each Condition.code must contain a valid ICD-10-CM code. Payer rules engines validate these codes against approved indication lists, coverage criteria, and medical-necessity policies.
Where it fails: According to a Pharmacy Times clinical review of prior authorization denials, incorrect ICD-10 coding is one of the most common and most preventable causes of PA denial. A payer requiring "severe persistent asthma, uncontrolled" (J45.50) may auto-deny "unspecified asthma" (J45.909). The difference is not clinical ambiguity—it is code specificity. A Surescripts survey found that 64% of specialty prescribers and 70% of specialty pharmacists see missing patient information as a top impediment to obtaining prior authorization, and two-thirds of prescribers report that improperly filled-out forms are the leading cause of delays.
Common specialty-drug examples:
| Drug class | Payer typically requires | Common wrong code | Result |
|---|---|---|---|
| Dupilumab (Dupixent) for severe asthma | J45.50 (severe persistent, uncontrolled) | J45.909 (unspecified) | Auto-deny: "diagnosis does not meet criteria" |
| Anti-VEGF for wet AMD | H35.3211 (exudative AMD, right eye) | H35.30 (unspecified macular degeneration) | Auto-deny: "diagnosis inconsistent with procedure" |
| PCSK9 inhibitor | E78.01 (familial hypercholesterolemia) | E78.5 (hyperlipidemia, unspecified) | Auto-deny: "diagnosis not on approved list" |
| Oncology biomarker-driven therapy | C79.82 (secondary malignant neoplasm) paired with biomarker code | Primary site code only, no biomarker | Auto-deny: "companion diagnostic result missing" |
What to fix: Hub teams and access technology vendors should build ICD-10 specificity validation into every PA submission. Cross-reference the submitted code against the payer's published medical policy for the requested drug. If the payer's criteria document lists a specific code or code range, do not accept a less-specific alternative.
The CO-146 denial code ("diagnosis was invalid for the dates of service reported") is triggered when ICD-10 codes are inactive, deleted, or truncated. Annual ICD-10 updates on October 1 create a predictable spike in CO-146 denials if EHR code libraries are not updated promptly.
2. Laboratory values and clinical documentation (Observation resources)
What happens: DTR Questionnaires often require lab results—HbA1c for GLP-1 therapy, ANA or CRP for immunology biologics, viral load for hepatitis C drugs, eGFR for SGLT2 inhibitors. These values populate Observation resources referenced in Claim.supportingInformation.
Where it fails: Three scenarios produce automated denials:
Missing observation. The EHR cannot locate a recent lab result. The DTR Questionnaire field is left empty. The payer's rules engine flags the submission as incomplete and returns a denial with reason "required clinical documentation missing."
Stale observation. The payer requires an HbA1c within the past 90 days. The only available result is 120 days old. The
Observation.effectiveDateTimefalls outside the payer's recency window. The denial states "clinical data does not meet recency requirements."Value below threshold. The payer requires HbA1c ≥ 7.0% for a GLP-1 PA. The submitted value is 6.8%. The payer's rules engine denies based on quantitative criteria.
In specialty oncology, the gap is particularly acute. Biomarker testing results—PD-L1 expression, HER2 status, EGFR mutation, microsatellite instability—must appear as coded Observation resources with LOINC codes. A narrative pathology report attached as a PDF does not satisfy a payer's automated rules engine.
What to fix: Hub intake workflows should require that lab values be captured with date, numeric result, LOINC code, and performing lab. PA submission systems should validate recency windows against the payer's medical policy before submission.
3. Step therapy and prior treatment history (Claim.supportingInformation → prior claims)
What happens: Payers require documentation that the patient has tried and failed preferred therapies before approving a non-preferred specialty drug. In FHIR, this evidence is typically submitted as Claim.supportingInformation with category values indicating prior treatment, or as MedicationStatement and MedicationRequest resources showing dispensing or administration history.
Where it fails: The most common failure modes are:
No pharmacy claims history in the EHR. The prescribing provider's EHR may not contain the patient's complete pharmacy claims history, especially if the patient filled prior prescriptions at a different pharmacy or under a different plan. The DTR engine cannot populate the step-therapy field, and the submission goes without it.
Wrong time window. A payer requires that the prior therapy was tried for a minimum of 12 weeks. The claims data shows only 4 weeks of fills. The
MedicationStatement.effectivePeriodis too short, triggering an automated denial.Adverse event documentation gap. When the step-therapy exception reason is "adverse event" rather than "inadequate response," the payer may require a coded adverse event using SNOMED CT or MedDRA. A free-text note stating "patient had a rash" does not satisfy a rules engine looking for a coded dermatological reaction.
A Molina Healthcare coverage policy for anti-VEGF therapy, revised in Q1 2026, illustrates the level of specificity required: "documentation of failure with (or documented intolerable adverse event) with 12 weeks of [prior agent]" with specific dose and duration requirements. When this criterion is encoded into a payer's automated PA system, an unsupported claim of prior therapy failure does not pass.
What to fix: Hub teams should collect structured step-therapy evidence at intake: drug name, NDC if available, start date, end date, outcome (adequate response, inadequate response, adverse event), and adverse event details with standard codes. Cross-reference against payer medical policy requirements before submission.
4. Prescriber specialty and taxonomy (Practitioner.qualification)
What happens: Many payers restrict certain specialty drugs to prescribers with specific board certifications. For example, a payer may require that anti-VEGF therapy be prescribed by a board-certified ophthalmologist or retina specialist, or that a CAR-T therapy be ordered by a hematologist/oncologist at a certified treatment center. In FHIR, this information maps to Practitioner.qualification resources and the ordering provider's NPI taxonomy codes.
Where it fails: The ordering provider's NPI record may not list the required taxonomy code, or the EHR may transmit a generic taxonomy (e.g., "Internal Medicine" 207R00000X instead of "Rheumatology" 207RR0500X). The payer's rules engine matches the taxonomy against an approved list. No match produces an automated denial.
The California Medical Association warned in April 2026 that Medi-Cal Rx would begin denying pharmacy claims and prior authorizations if the prescribing provider is not enrolled in Medi-Cal—a related but distinct problem of prescriber eligibility that compounds taxonomy validation failures.
What to fix: Before submitting a PA, verify the ordering provider's NPI taxonomy against the payer's prescriber-restriction criteria. If the provider's NPI record does not list the required taxonomy, either update the NPI record or confirm whether the payer accepts alternative documentation of specialty credentials.
5. Reauthorization and continuation evidence (Claim.supportingInformation → outcome documentation)
What happens: For chronic specialty therapies, payers require periodic reauthorization with evidence of continued benefit. This typically includes disease-severity measures, treatment-response documentation, and adherence records. In FHIR, these map to Observation resources for disease activity scores and Claim history for administration records.
Where it fails: Three patterns produce denials:
Stabilization treated as insufficient. Many oncology, immunology, and rare-disease therapies produce disease stabilization rather than improvement. Payer policies that require "documented improvement" will deny reauthorization when the evidence shows only stable disease, even though stabilization is clinically meaningful. This is a criteria-design problem, but it surfaces as an automated denial when the payer's rules engine evaluates an outcome score against a numeric threshold that requires improvement.
Missing administration records. Payers require documentation that the patient actually received the therapy. If administration records are not included in the reauthorization submission—dates, doses, route, and site of administration—the payer's system flags the submission as incomplete.
Expired authorization window. If the reauthorization is submitted after the current authorization period ends, the payer treats it as a new PA rather than a continuation, resetting the patient to initial-criteria requirements that may be harder to meet.
Molina Healthcare's Q1 2026 anti-VEGF reauthorization criteria illustrate the documentation burden: "reauthorization request is for the same eye(s) as initial authorization," "documentation of improvement or stabilization of disease state," "documentation of administration records showing dates and eye(s) administered, along with documentation of member compliance with treatment plan." Each of these requirements maps to specific FHIR fields that must be populated and transmitted.
What to fix: Establish a reauthorization calendar that initiates the process 60–90 days before the current authorization expires. Pre-populate the submission with the patient's treatment history, disease-activity trajectory, and compliance documentation.
The CMS-0057-F and CMS-0062-P regulatory context
Under CMS-0057-F, as of January 1, 2026:
- Payers must render PA decisions within 72 hours (standard) or 24 hours (expedited).
- Every PA denial must include a specific reason tied to coverage criteria—not generic "not medically necessary" language.
- Payers must publicly report PA metrics beginning with 2025 data (first reports were due March 31, 2026).
- FHIR-based Prior Authorization APIs must be operational by January 1, 2027.
CMS-0062-P, proposed April 14, 2026, would extend electronic PA to all drugs:
- Medical-benefit drug PA through the existing FHIR Prior Authorization API.
- Pharmacy-benefit drug PA through NCPDP SCRIPT and Real-Time Prescription Benefit standards.
- 24-hour decision timeframes for outpatient drugs.
- Drug-specific denial reasons and public reporting.
If finalized, most requirements take effect October 1, 2027. Public comments are open until June 15, 2026.
What manufacturer access teams should do now
Audit existing PA submissions for field completeness
Pull a sample of recent PA submissions across your top 10 payer-plan combinations. For each, check whether the following fields were populated at the specificity the payer's medical policy requires:
- ICD-10-CM diagnosis code (full specificity, current fiscal year)
- Lab values with LOINC codes and dates
- Step-therapy documentation with drug names, dates, and outcomes
- Prescriber taxonomy from NPI records
- Reauthorization outcome measures
Build a payer-criteria field map
For each specialty drug, create a matrix mapping payer medical-policy criteria to the specific FHIR resource fields required for automated adjudication. This map should be updated whenever a payer revises its criteria.
Test DTR Questionnaire responses
Before the January 2027 API deadline, test your hub or access platform's ability to complete DTR Questionnaires with data pulled from provider EHRs. Identify which fields the EHR consistently cannot populate and develop manual-capture workflows for those gaps.
Prepare for structured denial reasons
CMS-0057-F requires payers to provide specific denial reasons. Map these reasons to your field-level gap analysis. If the denial reason is "diagnosis code does not meet specificity requirements," the remediation is clear: resubmit with the correct ICD-10 code. If the denial reason is "step therapy documentation incomplete—prior trial duration insufficient," the remediation requires collecting additional claims data.
Engage payer technology teams
Manufacturer market access teams should engage payer interoperability teams now to understand how the payer's rules engine evaluates FHIR PA submissions. Ask for:
- The DTR Questionnaire templates for your drug.
- The automated-denial logic for missing or insufficient fields.
- The process for correcting and resubmitting denied requests.
What to monitor
- CMS-0062-P final rule. Expected late 2026 or early 2027. Will set the definitive timeline for drug PA API requirements.
- Payer DTR Questionnaire updates. Payers will revise their Questionnaires as they prepare for API compliance. Monitor for new required fields.
- EHR FHIR readiness. Not all EHRs support the full Da Vinci PAS workflow. Provider adoption will be uneven.
- Automated denial rates. As payers move from manual to automated adjudication, denial patterns will shift. Monitor denial reasons by field and payer.
Last updated: May 31, 2026. This article is for informational purposes only and does not constitute medical, legal, or reimbursement advice. It is not intended for individual patient treatment decisions.
Sources
- CMS. "CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F)." January 2024. https://www.cms.gov/priorities/burden-reduction/overview/interoperability/policies-regulations/cms-interoperability-prior-authorization-final-rule-cms-0057-f
- CMS. "2026 CMS Interoperability Standards and Prior Authorization for Drugs Proposed Rule (CMS-0062-P)." April 2026. https://www.cms.gov/newsroom/fact-sheets/2026-cms-interoperability-standards-prior-authorization-drugs-proposed-rule
- CMS. "Prior Authorization Application Programming Interface Workflow." https://www.cms.gov/files/document/prior-authorization-api-workflow-cms-0057-f.pdf
- Federal Register. "Medicare and Medicaid Programs: Interoperability Standards and Prior Authorization for Drugs." 91 FR 19891. April 14, 2026. https://www.federalregister.gov/documents/2026/04/14/2026-07205
- HL7 International. "Da Vinci Prior Authorization Support (PAS) FHIR Implementation Guide." https://build.fhir.org/ig/HL7/davinci-pas
- ONC. "Enhancing Healthcare Interoperability: Launching the DaVinci Prior Authorization Support (PAS) Test Kit." 2025. https://healthit.gov/blog/interoperability/enhancing-healthcare-interoperability-launching-the-davinci-prior-authorization-support-pas-test-kit
- Pharmacy Times. "Navigating Prior Authorization Denials: A Clinical Pharmacist's Approach to Appeals." 2025. https://www.pharmacytimes.com/view/navigating-prior-authorization-denials-a-clinical-pharmacists-approach-to-appeals
- Surescripts. "Inaccurate and Incomplete Data Delays Specialty Treatment for Patients and Is Top Stressor for Health Care Providers." https://surescripts.com/press-releases/inaccurate-and-incomplete-data-delays-specialty-treatment-patients-and-top-stressor-health-care-providers
- MedStates. "CO 146 Denial Code: Diagnosis Errors & Fixes Guide." https://www.medstates.com/co-146-denial-code
- Clearlink Partners. "CMS-0057-F & Prior Auth: Operating Under the New Standard." 2026. https://clearlinkpartners.com/blog/cms-0057-f-prior-authorization-operating-new-standard
- CMA. "DHCS to Require Diagnosis Codes on All Pharmacy Claims Beginning Fall 2026." April 2026. https://www.cmadocs.org/newsroom/news/view/ArticleId/51157/DHCS-to-require-diagnosis-codes-on-all-pharmacy-claims-beginning-fall-2026
- Molina Healthcare. "Eylea (Aflibercept) and Biosimilars Coverage Criteria C5674-A." Q1 2026 revision. https://www.molinahealthcare.com/providers/oh/medicaid/policies/-/media/Molina/PublicWebsite/PDF/Providers/oh/medicaid/policies/6-1-26-MHO-UM-C5674-A-Eylea-aflibercept-and-Biosimilars-508.pdf



