FDA interchangeability is one of the most misunderstood words in the biosimilar market. It sounds like a clinical verdict, a payer verdict, and a pharmacy verdict at the same time. It is none of those by itself. It is a regulatory designation that says a biosimilar has met the additional statutory requirements for substitution at the pharmacy level, subject to state law.
That distinction matters because commercial teams often treat interchangeability as if it automatically unlocks Humira-style substitution economics. It does not. A product can be interchangeable and still lose on formulary position, contracting, specialty-pharmacy routing, patient-support friction, or prescriber inertia.
What the FDA designation actually means
The FDA says a biosimilar must be highly similar to, and have no clinically meaningful differences from, the reference product. An interchangeable biosimilar must meet the biosimilar standard and additional requirements that support substitution. The FDA's biosimilar education page and the Purple Book are the practical source documents commercial teams should check before making claims about status.
The key sentence is not "same." The key sentence is "no clinically meaningful differences." Biosimilar approval is a totality-of-evidence review: analytical similarity, pharmacokinetics, immunogenicity, and any needed clinical data. Interchangeability adds evidence that switching between the reference product and the proposed interchangeable product does not create greater risk than staying on the reference product.
For commercial planning, that means FDA status answers one question: can the product be considered eligible for pharmacy-level substitution under federal law? It does not answer whether a payer will prefer it, whether a state allows substitution without prescriber notification, or whether a specialty pharmacy can operationalize the switch without hub disruption.
Why Purple Book status is necessary but not sufficient
The Purple Book is the working reference for biological product status. It tells teams the reference product, whether a product is biosimilar or interchangeable, and key licensing information. It does not tell you the net price, the preferred product on a payer's formulary, the specialty-pharmacy network, or the medical-policy criteria.
This is why a Purple Book read should be paired with a coverage read. A clean regulatory designation can still fail commercially if the product launches into a reference-product rebate wall or a payer has already selected a different biosimilar as preferred. The status is an entry ticket, not the finish line.
State substitution is its own layer
The FDA designation creates the federal pathway for substitution, but pharmacy substitution is implemented through state law. Some states require prescriber communication. Some require patient notification. Some impose record-keeping requirements. Those rules matter most when the product is distributed through retail pharmacy. For many specialty biologics, the operational site is specialty pharmacy or buy-and-bill, and the practical substitution point may be a benefit-design decision rather than a simple pharmacy counter event.
That is why the better commercial question is not "is it interchangeable?" It is "where does the switch decision happen?" In some categories, it happens in payer medical policy. In others, it happens in specialty pharmacy workflows. In others, it happens only after a prescriber writes the biosimilar because the channel does not behave like retail substitution.
The payer read
Payers can use interchangeability as a comfort signal, but they are usually optimizing for total cost, supply reliability, rebate structure, and administrative simplicity. A payer may prefer a non-interchangeable biosimilar if the net economics are stronger or if the manufacturer offers better operational support. Conversely, a payer may prefer the interchangeable product even without forcing automatic substitution, because the designation reduces provider pushback.
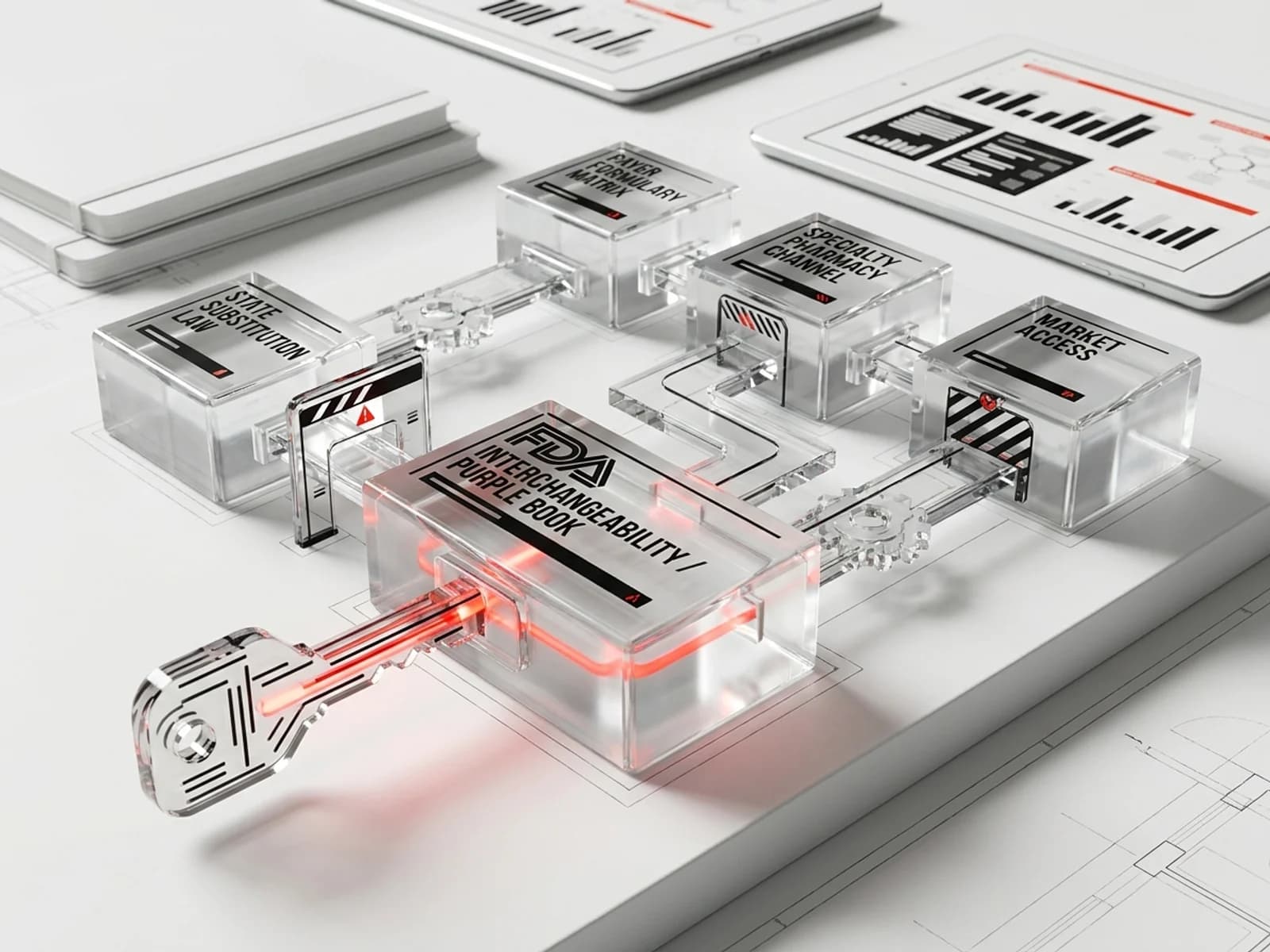
The practical payer matrix should include:
- reference product and all approved biosimilars;
- FDA status and Purple Book listing;
- pharmacy-benefit versus medical-benefit routing;
- preferred/non-preferred formulary status;
- prior-authorization and step-edit criteria;
- specialty-pharmacy restrictions;
- patient-support and copay program compatibility;
- state substitution friction if retail pharmacy is relevant.
That matrix is the commercial asset. The FDA designation is only one column.
What teams should say publicly
The safest public language is specific: "FDA has designated this product as interchangeable with the reference product" and "pharmacy substitution may be permitted subject to state law." Avoid saying "automatically substitutable" as a universal claim. Avoid implying that interchangeability means superior clinical performance. Avoid using the word "generic" for biologics, because the regulatory framework is different.
Interchangeability matters. It can reduce friction and support payer confidence. But the market share result still comes from payer contracting, channel execution, prescriber messaging, supply reliability, and patient-support continuity.
Sources
- FDA, Biosimilar and Interchangeable Biological Products: https://www.fda.gov/drugs/biosimilars/biosimilar-and-interchangeable-biological-products
- FDA Purple Book database: https://purplebooksearch.fda.gov/
- FDA, Scientific Considerations in Demonstrating Biosimilarity: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/scientific-considerations-demonstrating-biosimilarity-reference-product
- FDA, Considerations in Demonstrating Interchangeability With a Reference Product: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/considerations-demonstrating-interchangeability-reference-product