Xolair (omalizumab) is a recombinant DNA-derived humanized IgG1 monoclonal antibody that selectively binds to free immunoglobulin E (IgE), preventing IgE from binding to the high-affinity IgE receptor (FcεRI) on mast cells and basophils. This reduces surface-bound IgE, limits mediator release from the allergic response, and decreases FcεRI receptor density on basophils. The result is reduced allergic inflammation across multiple IgE-mediated diseases.
Co-developed by Genentech and Novartis, Xolair was first approved in the U.S. in 2003 for moderate-to-severe persistent allergic asthma. Its label has since expanded to chronic spontaneous urticaria (CSU, 2014), chronic rhinosinusitis with nasal polyps (CRSwNP, 2020), and IgE-mediated food allergy (2024). Novartis reported 2025 global Xolair sales of $1.723 billion.
In March 2025, the FDA approved Omlyclo (omalizumab-igec, Celltrion) as the first biosimilar to Xolair — and the first to carry an interchangeability designation. Omlyclo is approved for all four Xolair indications, with 75 mg/0.5 mL and 150 mg/1 mL prefilled syringes initially and a 300 mg/2 mL presentation approved in December 2025. Per a settlement agreement with Genentech, Omlyclo can enter the U.S. market as early as September 1, 2026. Additional omalizumab biosimilar candidates are in the pipeline from Teva (TEV-45779, FDA accepted March 2026) and Amneal/Kashiv (ADL-018, BLA submitted September 2025).
Access teams must navigate four distinct indications with different PA criteria and dosing tables, a medical-versus-pharmacy benefit split that varies by formulation and plan, an incoming interchangeable biosimilar with pharmacy-level substitution implications, and competing biosimilar pipeline entries.
Short answer
| Xolair (reference) | Omlyclo (biosimilar) | |
|---|---|---|
| Generic name | omalizumab | omalizumab-igec |
| Manufacturer | Genentech / Novartis | Celltrion USA |
| FDA first approval | June 2003 | March 7, 2025 |
| Interchangeability | N/A (reference product) | Yes — first and only interchangeable biosimilar to Xolair |
| Presentations | 75 mg/0.5 mL PFS/autoinjector, 150 mg/1 mL PFS/autoinjector, 300 mg/2 mL PFS/autoinjector, 150 mg vial | 75 mg/0.5 mL PFS, 150 mg/1 mL PFS, 300 mg/2 mL PFS |
| Administration | SC injection every 2 or 4 weeks | Same |
| Benefit channel | Medical benefit (provider-administered) or pharmacy benefit (self-administered PFS/autoinjector), varies by plan | Medical benefit (C9399 or J3590 until specific HCPCS assigned); pharmacy benefit for self-administered |
| HCPCS code | J2357 (Injection, omalizumab, 5 mg) | C9399 or J3590 (unclassified, until specific code assigned) |
| WAC (annual, Xolair) | ~$9,000–$144,000 depending on dose/frequency | Not yet announced; expected discount to Xolair |
| U.S. market entry | Available | Expected September 1, 2026 |
| PA required | Yes | Yes (same indications, similar criteria expected) |
FDA-approved indications (both products)
| Indication | Age | Dosing | Key PA criteria |
|---|---|---|---|
| Moderate-to-severe persistent allergic asthma | ≥6 years | 75–375 mg SC q2w or q4w, based on serum IgE and body weight | Positive skin test/in vitro reactivity to perennial aeroallergen; inadequately controlled on ICS ± controller meds |
| CRSwNP | ≥18 years | Per IgE/weight dosing table | Inadequate response to nasal corticosteroids; add-on maintenance |
| IgE-mediated food allergy | ≥1 year | Per IgE/weight dosing table (up to 600 mg q2w) | Confirmed IgE-mediated food allergy; used with food avoidance; epinephrine access |
| CSU | ≥12 years | 150 or 300 mg SC q4w (not IgE/weight-based) | Symptomatic despite H1 antihistamine treatment |
Medical vs. pharmacy benefit routing
Xolair benefit routing is one of the more complex in specialty pharmacy because it depends on formulation, administration setting, and plan design.
Provider-administered (medical benefit)
- Lyophilized 150 mg vial: reconstituted and injected by a healthcare provider
- Any presentation given in a clinical setting
- Billed under HCPCS J2357 (5 mg per unit)
- PA under medical benefit drug policies
Self-administered (pharmacy benefit)
- Prefilled syringe (PFS) and autoinjector formulations: after the provider determines self-administration is appropriate
- UnitedHealthcare (effective July 2025): self-administered PFS and autoinjector processed under pharmacy benefit
- Blue Cross Blue Shield of Illinois (effective April 2025): self-administered formulations moved to pharmacy benefit, with medical benefit coverage only when administration in a healthcare setting is medically necessary
- Blue Shield of California: pharmacy benefit for self-administered PFS; medical benefit for provider-administered
- Medicaid plans vary: some cover under pharmacy benefit (e.g., Neighborhood Health Plan of RI covers Medicaid under pharmacy, commercial/Medicare under medical)
Self-administration criteria
Before a patient can self-administer Xolair or Omlyclo, the label requires:
- No prior history of anaphylaxis (to omalizumab or other agents; for food allergy, anaphylaxis to non-food agents)
- At least 3 doses administered under healthcare provider guidance with no hypersensitivity reactions
- Patient or caregiver can recognize anaphylaxis symptoms
- Patient or caregiver can treat anaphylaxis appropriately
- Patient or caregiver can perform subcutaneous injections with proper technique
Indication-specific PA criteria
Allergic asthma (moderate-to-severe persistent)
UnitedHealthcare (PA-Med-Nec-Xolair, effective July 2025) and most major payers require:
- Age ≥6 years
- Diagnosis of moderate-to-severe persistent asthma
- Positive skin test or in vitro reactivity to a perennial aeroallergen
- Inadequate control on inhaled corticosteroids (ICS) with documented compliance
- Prior trial or documented contraindication to at least one controller medication (LABA, LTRA, or theophylline)
- Total serum IgE ≥30 IU/mL (required for dosing)
- Prescribed by allergist, immunologist, or pulmonologist (many plans)
- Not receiving concurrent Dupixent, Nucala, Cinqair, Fasenra, or Tezspire for the same indication
- Initial authorization: typically 12 months
Chronic spontaneous urticaria (CSU)
- Age ≥12 years
- Diagnosis of CSU
- Symptomatic despite H1 antihistamine treatment
- Dose: 150 or 300 mg q4w (not IgE/weight-based)
- Initial authorization: typically 6 months
- Reauthorization requires documentation of continued response
CRSwNP
- Age ≥18 years
- Diagnosis of CRSwNP confirmed by imaging or endoscopy
- Inadequate response to nasal corticosteroids
- Many plans require prior trial of oral corticosteroid
- Add-on maintenance treatment with continued nasal corticosteroid use
- Not receiving concurrent Dupixent, Nucala, Cinqair, Fasenra, or Tezspire for the same indication
IgE-mediated food allergy
- Age ≥1 year
- Body weight ≥10 kg
- Pre-treatment serum IgE ≥30 IU/mL (for dosing)
- Used in conjunction with food allergen avoidance
- Patient has epinephrine access
- Prescribed by an allergist (most plans)
- Dosing based on IgE/weight table (up to 600 mg q2w for higher weights/IgE levels)
- Authorization: typically 12 months
HCPCS coding
| Code | Description | Application |
|---|---|---|
| J2357 | Injection, omalizumab, 5 mg | Xolair, provider-administered, medical benefit |
| Q5154 | Injection, omalizumab-igec, 5 mg | Omlyclo, provider-administered, medical benefit (assigned by some payers effective October 2025) |
| C9399 | Unclassified drugs or biologicals | Omlyclo (interim code, use Q5154 when available) |
| J3590 | Unclassified biologics | Omlyclo (alternative interim code) |
Billing unit example for Xolair: a 300 mg dose = 60 billable units of J2357. Quantity limits per payer: typically 2 PFS/autoinjectors per 28 days for 75 mg, 4 per 28 days for 150 mg, and 2 per 28 days for 300 mg.
Omlyclo interchangeability and pharmacy substitution
What interchangeability means
The FDA's interchangeability designation means that Omlyclo can be substituted for Xolair at the pharmacy level without requiring prescriber authorization. This is distinct from a standard biosimilar designation, which requires a new prescription for the biosimilar.
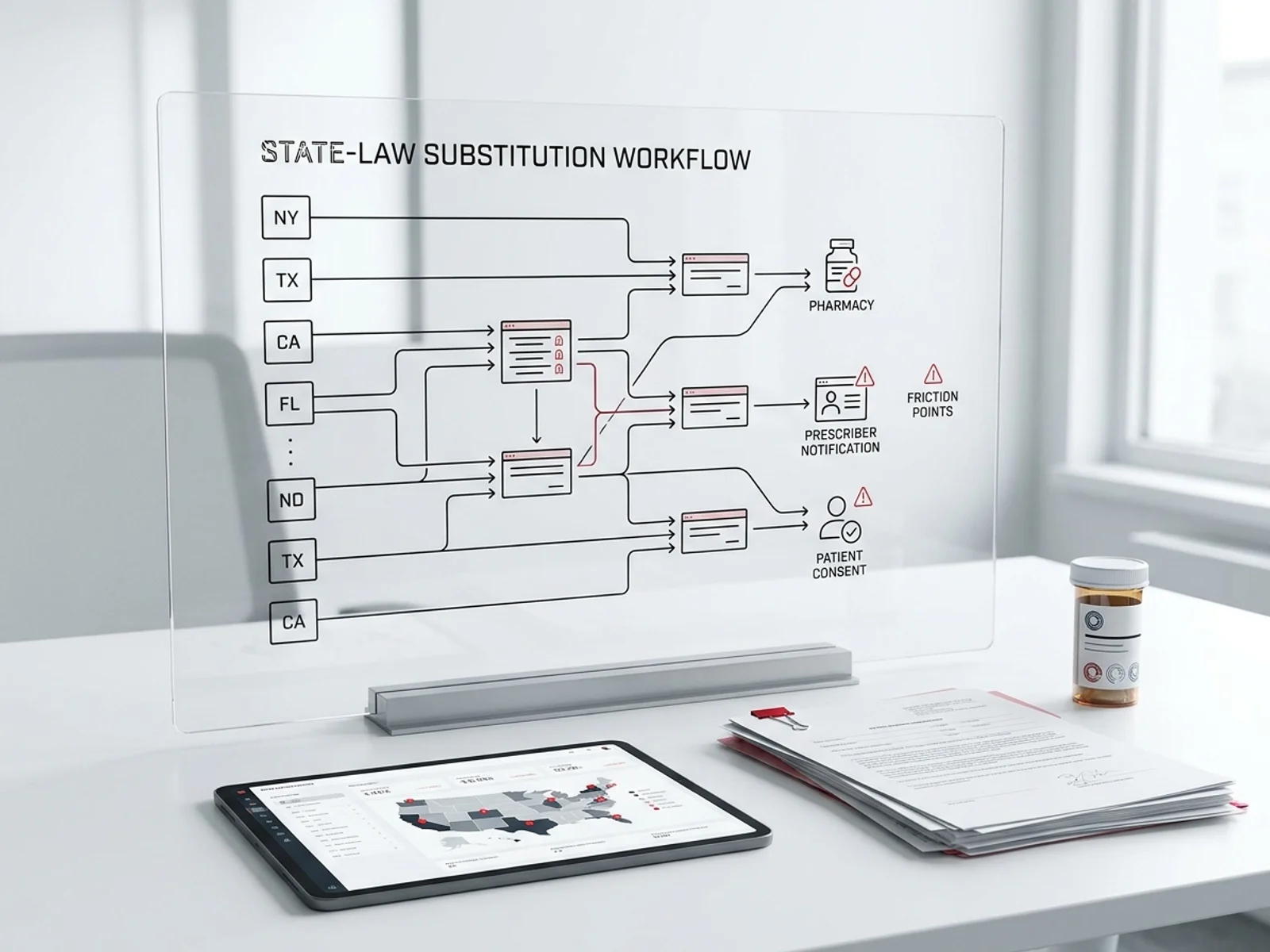
State substitution laws
Federal law permits pharmacy-level substitution for interchangeable biosimilars, but state laws govern notification and consent:
- Most states allow automatic substitution with post-hoc notification to the prescriber
- Some states require patient notification before or after substitution
- Four states (Alabama, Indiana, South Carolina, and Washington) restrict interchangeability substitution entirely, as of early 2026
- Access teams should verify state-specific requirements when Omlyclo launches
Formulary implications
When Omlyclo enters the market in September 2026, PBMs and payers are expected to position it preferentially on formularies, potentially moving Xolair to non-preferred or requiring step therapy through Omlyclo first. Key considerations:
- Pharmacy benefit formulations (PFS) will be the primary substitution target because pharmacists control dispensing
- Medical benefit formulations (vials, provider-administered) require a prescription change, not pharmacy substitution
- Plans may implement different tiering for Xolair vs. Omlyclo, with lower copay for the biosimilar
- The "grandfathering" question: stable patients on Xolair may face payer-driven switching to Omlyclo at reauthorization
Omlyclo approval evidence
The FDA approval and interchangeability designation were supported by:
- Phase 3 trial (NCT04426890): 619 adult patients with CSU randomized to Omlyclo 300 mg, Omlyclo 150 mg, Xolair 300 mg, or Xolair 150 mg every 4 weeks for 12 weeks
- Primary endpoint: Change from baseline in weekly itch severity score (ISS7) at week 12 — Omlyclo 300 mg demonstrated equivalent efficacy to Xolair 300 mg (treatment difference 0.77 [95% CI, -0.37, 1.90])
- Switching study: From week 12, Xolair 300 mg patients were re-randomized 1:1 to switch to Omlyclo or continue Xolair. Switching had no impact on treatment outcomes through week 40
- Extrapolation: Approval for allergic asthma, CRSwNP, and food allergy was extrapolated from CSU data, supported by comprehensive analytical and PK/PD data
Biosimilar pipeline competition
| Biosimilar | Sponsor | Status | Notes |
|---|---|---|---|
| Omlyclo (omalizumab-igec) | Celltrion | FDA approved March 2025; interchangeable | Market entry September 2026 |
| ADL-018 | Amneal / Kashiv BioSciences | BLA submitted September 2025; FDA accepted | Amneal holds U.S. commercial rights; anticipating 2026 launch |
| TEV-45779 | Teva | FDA accepted March 2026 | Phase 3 completed May 2024; in regulatory review |
| Others | Aurobindo, Glenmark | Early-stage | No announced FDA filings |
Celltrion's first-to-market advantage with interchangeability gives Omlyclo a significant commercial edge. However, Amneal/Kashiv and Teva entries could further erode Xolair's market share and create multi-biosimilar formulary competition.
Patient support programs
Xolair Access Solutions (Genentech)
- Benefits investigation and prior authorization support
- Practice forms and letter of medical necessity templates
- Xolair copay program for commercially insured patients
- Patient Assistance Program for uninsured/underinsured patients
- Available at www.xolairhcp.com
Omlyclo (Celltrion)
- Patient support program details expected closer to September 2026 launch
- Celltrion USA will market and distribute Omlyclo exclusively in the U.S.
Transition considerations
When Omlyclo launches, access teams should prepare for:
- New PA criteria: Payers will establish Omlyclo-specific criteria, likely mirroring Xolair criteria but potentially with step-therapy requirements
- Switching documentation: Patients switching from Xolair to Omlyclo at payer request may need documentation of stable disease on the reference product
- Copay program differences: Omlyclo's copay program terms have not yet been announced
- Formulary exclusion risk: Xolair may face formulary exclusion or non-preferred tiering as Omlyclo gains preferred status
Access friction points
- Benefit routing complexity: Xolair's move from medical to pharmacy benefit for self-administered formulations creates routing confusion. Different plans have different effective dates and criteria. Access teams must verify benefit channel before each PA
- IgE-based dosing tables: For asthma, CRSwNP, and food allergy, the dose depends on both serum IgE and body weight. The dosing table is complex and varies by age. PA submissions must include current IgE level and weight for correct dose approval
- Exclusion of concurrent biologics: Payers uniformly exclude concurrent use of Xolair/Omlyclo with Dupixent, Nucala, Cinqair, Fasenra, or Tezspire for the same indication. Document that no concurrent biologic is prescribed
- Anaphylaxis risk and initial doses: The first 3 doses must be administered under healthcare provider supervision. Payer criteria for self-administration require documented completion of these 3 supervised doses
- Biosimilar transition uncertainty: With Omlyclo launching September 2026 and two additional biosimilar candidates in the pipeline, formulary positioning will shift rapidly. Access teams should monitor PBM formulary updates quarterly
- Quantity limits mismatch: Some plans impose quantity limits that may not align with higher-weight or higher-IgE dosing requirements (e.g., up to 600 mg q2w for food allergy). Override criteria should be prepared
Sources
- Xolair prescribing information. Genentech, Inc. Revised February 2024. https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=7f6a2191-adfb-48b9-9bfa-0d9920479f0d
- Omlyclo prescribing information. Celltrion USA, Inc. Revised December 2025 (300 mg supplement). https://www.accessdata.fda.gov/drugsatfda_docs/label/2026/761399s004lbl.pdf
- FDA approves Omlyclo (omalizumab-igec), a biosimilar to Xolair (omalizumab). FDA. March 7, 2025. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-omlyclo-omalizumab-igec-biosimilar-xolair-omalizumab
- Celltrion gains first omalizumab biosimilar approval. Biosimilars Review & Report. March 11, 2025. https://biosimilarsrr.com/2025/03/11/celltrion-gains-first-omalizumab-biosimilar-approval
- FDA and EMA accept Teva's omalizumab biosimilar applications. Venable BiologicsHQ. March 31, 2026. https://biologicshq.com/fda-and-ema-accept-tevas-omalizumab-biosimilar-applications
- Kashiv BioSciences omalizumab biosimilar application submitted to FDA. Goodwin/Big Molecule Watch. September 2025. https://www.goodwinlaw.com/en/insights/blogs/2025/10/kashiv-biosciences-omalizumab-biosimilar-application-submitted-to-fda-accepted-by-ema
- UnitedHealthcare. Xolair prior authorization/medical necessity. Program 2025 P 2238-10. Effective July 2025. https://www.uhcprovider.com/content/dam/provider/docs/public/prior-auth/drugs-pharmacy/commercial/r-z/PA-Med-Nec-Xolair.pdf
- Anthem/Elevance Health. Omlyclo/Xolair clinical criteria. CC-0033. Revised July 2025. https://files.providernews.anthem.com/6558/CC-0033_Pub-07-01-2025-(redline).pdf
- Blue Shield of California. Omalizumab (Xolair) medical benefit drug policy. Effective February 2026. https://www.blueshieldca.com/content/dam/bsca/en/provider/docs/medi-cal-med-benefit-drug-policy/omalizumab-Xolair-MCAL-UMRx-provider.pdf
- Health Net. Omalizumab (Xolair, Omlyclo) clinical policy. CP.PCH.49. https://www.healthnet.com/content/dam/centene/policies/pharmacy-policies/pch/CP.PCH.49.pdf
- Aetna Better Health NJ Medicaid. Xolair-Omlyclo coverage policy. Effective September 2025. https://www.aetnabetterhealth.com/content/dam/aetna/medicaid/pdfs/formulary/guidelines/Xolair-Omlyclo-Aetna-NJ-Medicaid-Policy-ua.pdf