Tezspire (tezepelumab-ekko, Amgen/AstraZeneca) is a first-in-class thymic stromal lymphopoietin (TSLP) blocker approved for add-on maintenance treatment of severe asthma and, since October 2025, chronic rhinosinusitis with nasal polyps (CRSwNP) in patients aged 12 years and older. Unlike eosinophilic-targeted biologics (Nucala, Fasenra, Cinqair) or anti-IgE therapy (Xolair), Tezspire acts upstream at the alarmin level, making it the only severe asthma biologic without a biomarker requirement for initiation. That positioning drives both its clinical appeal and its payer step-therapy complexity.
This guide covers Tezspire's formulary positioning, step-therapy hierarchies, benefit-channel routing, HCPCS coding, and patient support programs for access teams navigating severe asthma and CRSwNP coverage.
Short answer
| Tezspire (vial / prefilled syringe) | Tezspire (prefilled pen) | |
|---|---|---|
| Drug class | TSLP blocker; human IgG2-lambda monoclonal antibody | Same |
| Manufacturer | Amgen Inc. / AstraZeneca | Same |
| FDA indications | Severe asthma (add-on, age 12+); CRSwNP (add-on, age 12+) | Same |
| Administration | SC injection by healthcare provider | SC self-injection by patient/caregiver after training |
| Dosing | 210 mg SC every 4 weeks | Same |
| Benefit channel | Medical benefit (vial, PFS) | Pharmacy benefit (most plans) |
| HCPCS code | J2356 (Injection, tezepelumab-ekko, 1 mg) | N/A — pharmacy benefit |
| WAC list price | ~$4,850 per 210 mg dose (estimated) | Same |
| PA required | Yes, all major commercial and Medicare plans | Yes |
| Reauthorization | 12 months with documented clinical improvement | Same |
Indication-specific coverage criteria
Severe asthma
Severe asthma is the original Tezspire indication, and payer PA criteria are well established across UHC, Cigna, Aetna, Mass General Brigham, and FEP Blue:
- Diagnosis: severe asthma confirmed by an allergist, pulmonologist, or immunologist, age 12+
- Inadequate control despite optimized standard therapy: minimum 3-month trial of ICS plus LABA at maximally indicated doses. Some plans also require failure of an additional controller (LTRA, LAMA, or theophylline). Mass General Brigham requires documentation of hospitalization or emergency care within the past year, or objective measures of poor control.
- Step therapy — biologic sequencing: most plans require trial and failure of at least one preferred asthma biologic before Tezspire. UHC requires failure of Dupixent unless contraindicated. Ambetter/Centene requires a 4-month trial of Dupixent at maximally indicated doses. Moda Health (Prime Therapeutics) requires Medicaid members to fail two of Nucala, Dupixent, or Xolair before Tezspire.
- No concurrent asthma biologics: Tezspire must not be combined with Cinqair (reslizumab), Dupixent (dupilumab), Fasenra (benralizumab), Nucala (mepolizumab), or Xolair (omalizumab) for the same indication.
Chronic rhinosinusitis with nasal polyps (CRSwNP)
The CRSwNP indication was approved in October 2025 based on the WAYPOINT Phase III trial. Payer policies have been updating through early 2026:
- Diagnosis: CRSwNP with bilateral nasal polyps confirmed by nasal endoscopy, plus two or more symptoms for >12 weeks (nasal obstruction, mucopurulent discharge, facial pain/pressure, reduction in smell). UHC also requires CT confirmation (maxillofacial).
- Inadequate response to intranasal corticosteroids: at least a 4-week trial of an intranasal corticosteroid (fluticasone, mometasone, triamcinolone). Prime Therapeutics (Boeing) accepts failure of one intranasal corticosteroid or Sinuva (mometasone implant).
- Step therapy: Ambetter requires a 4-month trial of Dupixent for CRSwNP before Tezspire. UHC added CRSwNP-specific criteria in its February 2026 policy update.
- Prescriber specialty: allergist, immunologist, or otolaryngologist (ENT) — most plans require specialist involvement.
- Add-on therapy attestation: Tezspire must be used in combination with an intranasal corticosteroid, not as monotherapy.
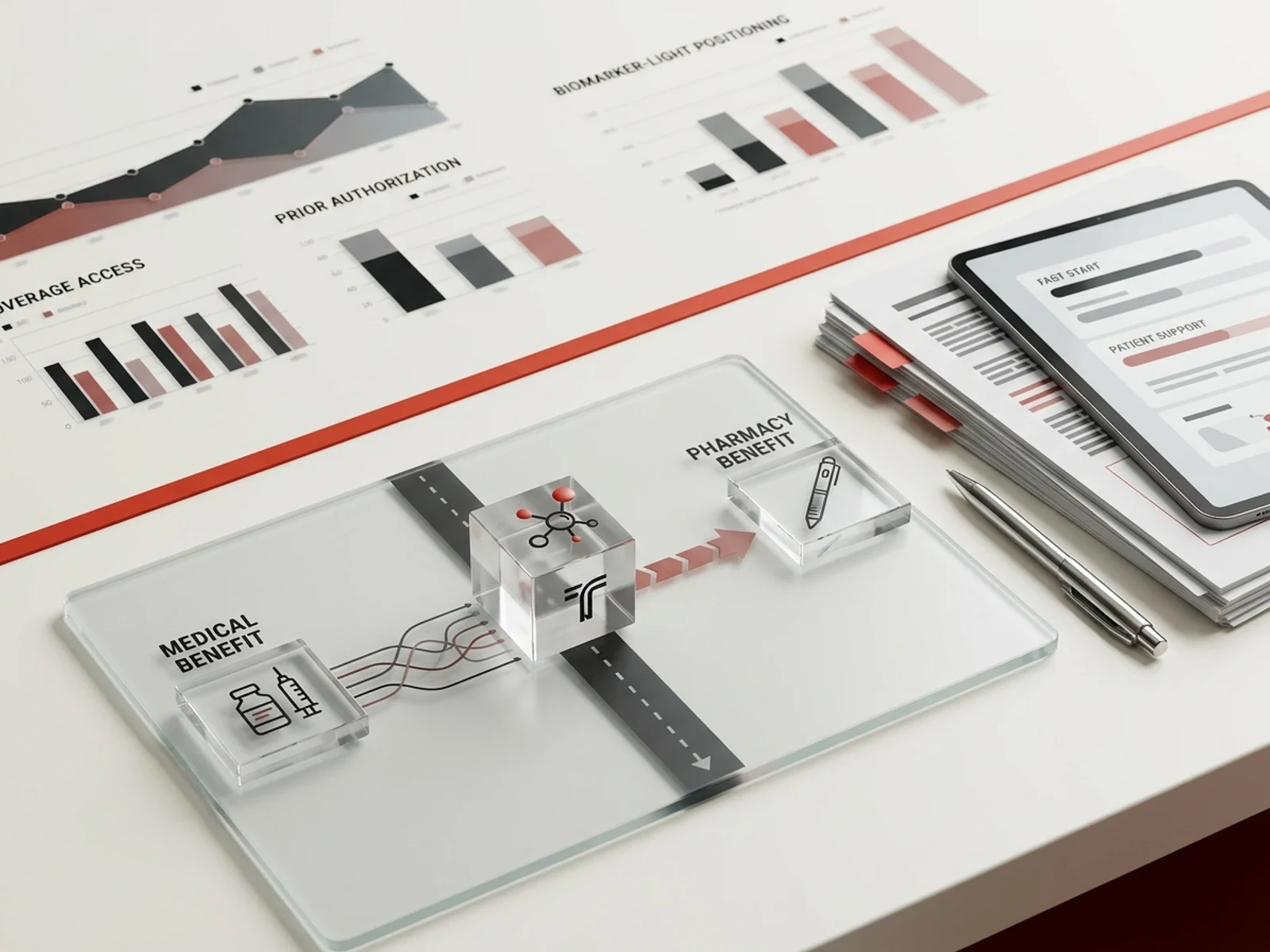
Biomarker-light positioning and payer implications
Tezspire's unique clinical advantage is that it does not require a specific biomarker (blood eosinophil count, FeNO, or IgE level) for initiation. This differentiates it from:
- Nucala / Fasenra / Cinqair: require elevated eosinophils (typically ≥150 or ≥300 cells/μL)
- Xolair: requires elevated IgE or allergic sensitization
- Dupixent: no strict biomarker requirement but labeled for eosinophilic or type 2 asthma
Despite the biomarker-light label, payers still impose step edits requiring failure of biomarker-restricted agents first. Access teams should document:
- Blood eosinophil count and FeNO results even though Tezspire does not require them, because payers often ask for phenotype characterization during PA review
- Reasons why biomarker-specific agents failed (lack of efficacy, adverse effects, or inability to meet the specific threshold)
- That the patient's asthma phenotype does not contraindicate upstream TSLP blockade
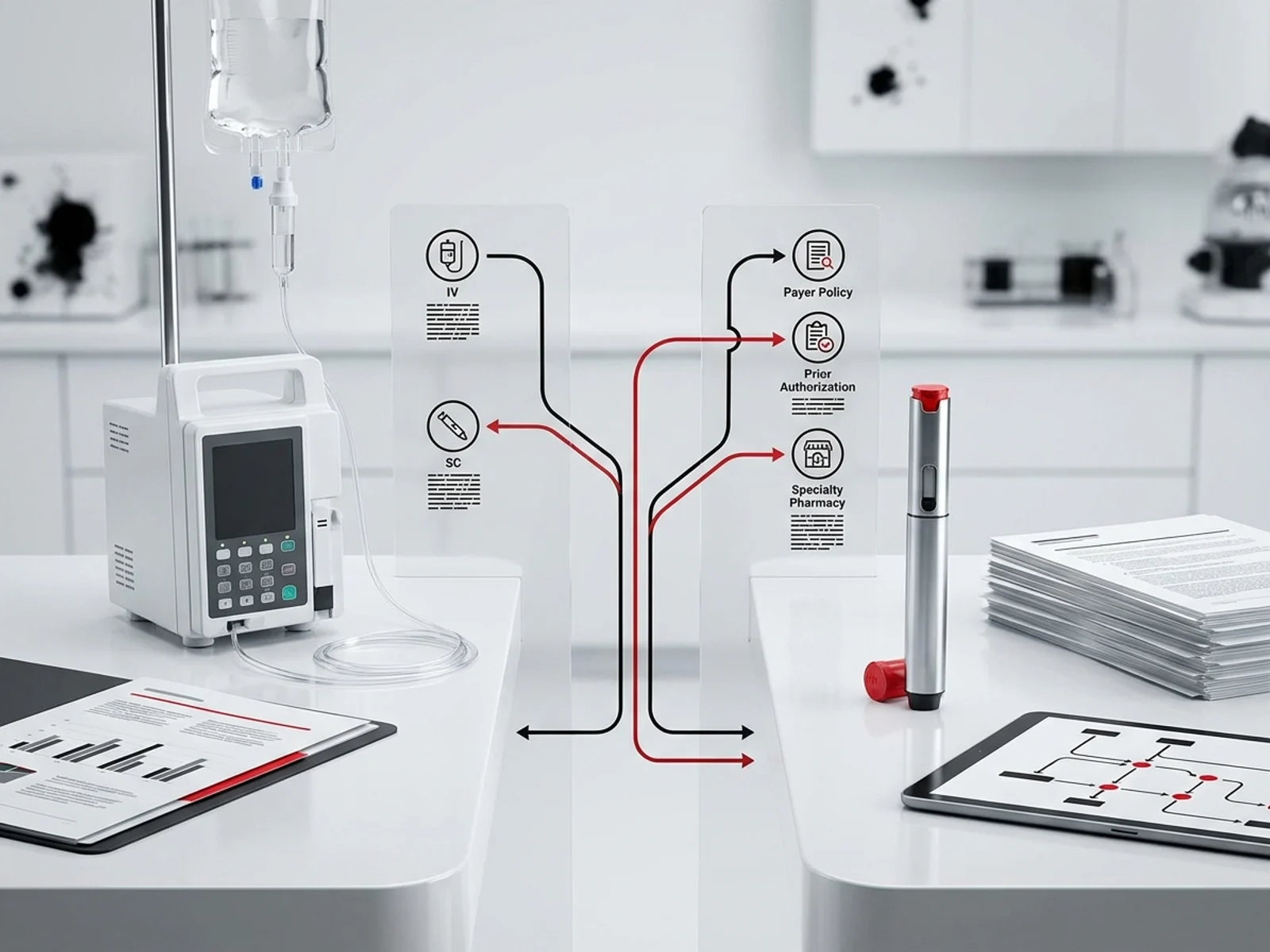
Medical vs pharmacy benefit routing
Tezspire's benefit channel depends on the formulation:
Medical benefit (vial and prefilled syringe)
- Administered by a healthcare provider in an office, clinic, or infusion center
- Billed under medical benefit using HCPCS J2356
- Site-of-care edits apply: UHC, Medical Mutual of Ohio, and others restrict administration to non-hospital facility-based locations (provider's office, free-standing ambulatory infusion center, home infusion)
- Requires buy-and-bill or specialty distribution
Pharmacy benefit (prefilled pen)
- Self-administered by the patient after proper training and provider determination
- Dispensed through contracted specialty pharmacies
- Mass General Brigham moved Tezspire from medical benefit to pharmacy benefit for its commercial and exchange plans effective January 2026
- UHC notes that the prefilled pen is obtained under pharmacy benefit "unless otherwise specified in the member's benefit plan documents," with a California exception for delegated provider groups where it may remain on medical benefit
Routing implications for access teams
- Verify the prescribed formulation matches the plan's expected benefit channel
- A new PA is typically required when switching between medical benefit (vial/PFS) and pharmacy benefit (pen)
- Confirm specialty pharmacy network for pen formulation — some plans designate a single specialty pharmacy
HCPCS coding and billing
Tezspire uses a permanent HCPCS code:
- J2356: Injection, tezepelumab-ekko, 1 mg (1 billable unit = 1 mg)
- Bill 210 units per dose (210 mg administered every 4 weeks)
- NDC examples: 55513-0123-xx (prefilled pen), 55513-0112-xx (prefilled syringe), 55513-0100-xx (vial)
- JW/JZ modifier: required for Medicare Part B claims for single-use containers
- Administration CPT: 96372 (SC/IM injection) for provider-administered doses; consult payer for correct code
- ICD-10 codes: J45.40–J45.52 (severe asthma), J33.0–J33.9 (nasal polyps/CRSwNP), J31.0 (chronic rhinitis), J32.0–J32.9 (chronic sinusitis)
2026 payer formulary positioning
UnitedHealthcare / Optum Rx
Tezspire is subject to prior authorization under UHC's Commercial Medical Benefit Drug Policy (effective February 1, 2026). For severe asthma, Tezspire requires prior failure of Dupixent. For CRSwNP, Tezspire requires documentation of endoscopic polyps, CT confirmation, and intranasal corticosteroid failure. Reauthorization requires documented improvement in exacerbation frequency, rescue medication use, FEV1, or symptom severity.
Cigna
Cigna's National Formulary Coverage Policy requires Tezspire to be prescribed by a specialist (allergist, pulmonologist, or immunologist). Step therapy requires failure of at least one preferred biologic (Dupixent preferred for most plans) before Tezspire. Reauthorization requires continued ICS/LABA use alongside Tezspire.
Aetna
Aetna's Clinical Policy Bulletin (CPB 1003) covers Tezspire as medically necessary for severe asthma when criteria are met. Last reviewed January 27, 2026, with next review May 28, 2026. Aetna references the same step-therapy logic as UHC and Cigna.
FEP Blue
FEP Blue covers Tezspire with prior authorization. Quantity limits: 210 mg/1.91 mL (3 units per 84 days for vial/syringe formulations). Patients age 18+ must have tried the preferred product(s) per formulary appendix. Authorization duration: 12 months.
Mass General Brigham Health Plan
Moved Tezspire to pharmacy benefit effective January 2026. CRSwNP criteria added effective April 2026. Specialty pharmacy required. Prior authorization required for all formulations.
TEZSPIRE Together patient support
Fast Start program
For patients whose insurance requires prior authorization or does not yet cover Tezspire:
- Patients can receive Tezspire at no cost for up to 12 doses (prefilled syringe or pen) within 24 months of first shipment
- The provider must submit the PA within 30 days of first shipment; if PA is not submitted, the patient is no longer eligible
- Available for commercially insured patients only
Co-pay support
- Commercially insured patients may pay as little as $0 per dose
- Up to $100 per month for in-office administration costs (prefilled syringe only)
- Not valid for residents of Massachusetts or Rhode Island (injection administration support)
Patient Assistance Program
For uninsured patients or those with Medicare affordability gaps:
- Provides Tezspire at no cost to qualifying patients
- Eligibility criteria apply
- Contact: 1-888-TEZSPIRE (1-888-897-7473), Monday–Friday, 8:00 AM–8:00 PM ET
Coverage data
According to TEZSPIRE Together (based on MMIT data, February 2025):
- 90% of commercially insured patients have access to Tezspire
- 89% of commercially insured patients are covered for the prefilled pen (at-home)
- 90% of Medicare patients are covered for the prefilled syringe (in-office)
Reauthorization documentation
Across major payers, Tezspire reauthorization every 12 months requires:
- Positive clinical response documented by at least one of:
- Decreased frequency of asthma exacerbations (requiring systemic corticosteroids or increased ICS dose)
- Decreased rescue medication utilization
- Increase in percent predicted FEV1 from pretreatment baseline
- Reduction in asthma-related symptoms (wheezing, shortness of breath, coughing, sleep disturbance)
- For CRSwNP: decreased nasal congestion, improved smell, reduction in nasal polyp size
- Continued background therapy: ICS plus LABA continued for asthma; intranasal corticosteroid continued for CRSwNP
- No concurrent biologics: Tezspire must not be combined with other asthma/CRSwNP biologics
- Prescriber attestation: ongoing monitoring and periodic reassessment of continued need
Documentation checklist for PA submission
- ICD-10 codes: J45.40–J45.52 (severe asthma), J33.0 (nasal polyp of nasal cavity), J32.0–J32.9 (chronic sinusitis), J31.0 (chronic rhinitis)
- Disease severity documentation: exacerbation history (hospitalizations, ER visits, oral corticosteroid bursts), pulmonary function tests (FEV1), ACT or ACQ scores
- Prior treatment history: drug name, dose, start/stop dates, and reason for discontinuation for each prior therapy — especially ICS/LABA, and any prior asthma biologic
- Biomarker data: blood eosinophil count, FeNO, total IgE (not required for Tezspire but often requested during PA review)
- Specialist attestation: prescribed by or in consultation with an allergist, pulmonologist, or immunologist (CRSwNP: allergist, immunologist, or ENT)
- HBV screening: not a labeled requirement for Tezspire but often included in payer PA forms
- Formulary exception letter (if non-preferred): cite reasons preferred alternatives are inappropriate, including prior biologic failures, contraindications, or biomarker-ineligible phenotype
Key takeaways for access teams
- Tezspire is the only severe asthma biologic without a biomarker requirement, but payers still impose step therapy requiring failure of biomarker-restricted agents — document why those agents failed or were inappropriate.
- Benefit channel depends on formulation: vial and prefilled syringe route through medical benefit (J2356); prefilled pen routes through pharmacy benefit. Confirm the correct channel before filing PA.
- CRSwNP is a new indication as of October 2025: payer policies are still updating. Check for plan-specific CRSwNP criteria.
- Fast Start provides up to 12 free doses while PA is pending — but the provider must submit PA within 30 days.
- Reauthorization requires documented clinical response across objective measures (exacerbations, FEV1, rescue use) and continued background controller therapy.
Sources
- FDA. Tezspire (tezepelumab-ekko) Prescribing Information. BLA 761224. https://www.accessdata.fda.gov/drugsatfda_docs/label/2023
- UnitedHealthcare. Tezspire (Tezepelumab-Ekko) Commercial Medical Benefit Drug Policy. Policy 2026D0110K. Effective 02/01/2026. uhcprovider.com
- UnitedHealthcare. Tezspire Prior Authorization/Medical Necessity. uhcprovider.com
- Cigna. Multiple Sclerosis / Respiratory – Tezspire Prior Authorization Policy. CNF. static.cigna.com
- Aetna. Tezepelumab-ekko (Tezspire) Clinical Policy Bulletin. CPB 1003. Last review 01/27/2026. aetna.com
- FEP Blue. Tezspire (tezepelumab-ekko) Pharmacy Policy. 5.45.015. Effective 01/01/2026. fepblue.org
- Mass General Brigham Health Plan. Tezspire (tezepelumab-ekko) PA Policy. Effective 04/01/2026. resources.massgeneralbrighamhealthplan.org
- Blue Shield of California. Tezepelumab-ekko (Tezspire) Medical Benefit Drug Policy. Effective 03/01/2026. blueshieldca.com
- Ambetter Health. Tezepelumab-ekko (Tezspire) Clinical Policy. HIM.PA.176. ambetterhealth.com
- Medical Mutual of Ohio. Tezspire Corporate Drug Policy. CDP-022201. medmutual.com
- Moda Health / Prime Therapeutics. Tezspire Medical Necessity Criteria. MODA-P0650. modahealth.com
- Amgen/AstraZeneca. TEZSPIRE Together Support Program. tezspire.com/paying-for-tezspire
- Amgen/AstraZeneca. Tezspire HCP Coverage Access Support. tezspirehcp.com/severe-asthma/support-and-resources
- Amgen/AstraZeneca. Tezspire Billing and Coding Guide. HCPCS J2356. tezspirehcp.com
- Prime Therapeutics (Boeing). Tezspire PAQL Program Summary. Effective 04/01/2026. myprime.com