The access gap in specialty pharma is not that the internet lacks drug pages. It is that most pages stop where launch teams start. A manufacturer page explains the label. A coupon page explains a retail discount. A payer policy explains one plan's rules. None of those alone tells a patient-support team, market-access lead, or specialty pharmacy what will actually happen when a prescription enters the system.
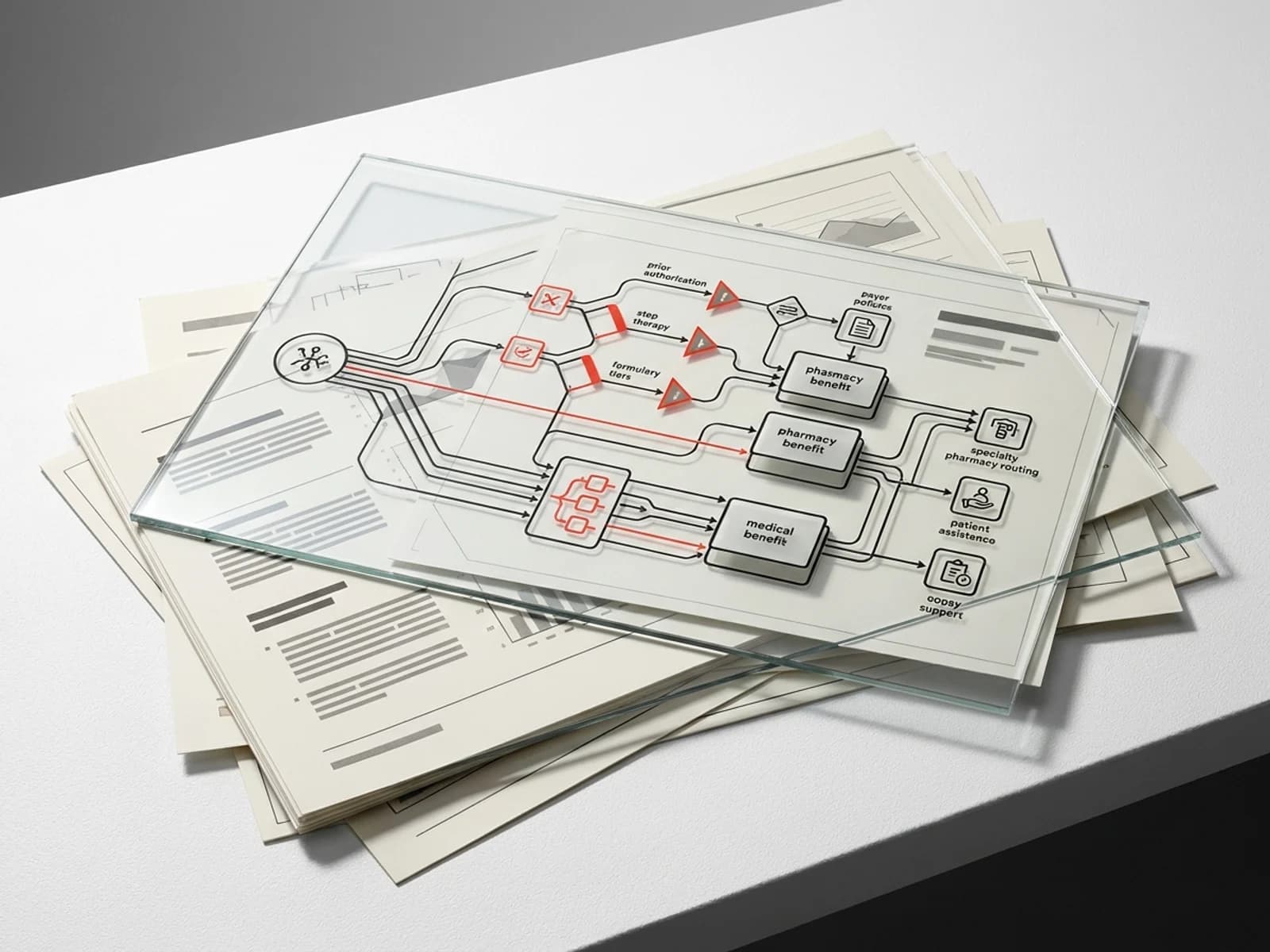
That is why the useful artifact is a payer coverage matrix. Not a broad "covered or not covered" table, but a workflow map that connects benefit routing, formulary tier, prior authorization, step therapy, specialty pharmacy, patient assistance, renewal timing, and alternatives.
Start with the benefit channel
The first column should be benefit channel: pharmacy benefit, medical benefit, or mixed. This decides who controls the transaction. Pharmacy-benefit drugs move through PBM formulary logic, NCPDP transactions, pharmacy claims, specialty pharmacy routing, and copay accumulator exposure. Medical-benefit drugs move through buy-and-bill, HCPCS coding, site-of-care policy, medical necessity review, and provider inventory risk.
The same drug can look commercially different depending on indication and site of care. A simple "covered" flag hides that difference. For specialty drugs, benefit routing is often the most important access variable.
Capture utilization management, not just tier
Formulary tier is visible and easy to summarize. It is also incomplete. Prior authorization determines whether the prescription can move. Step therapy determines what failure history must be documented. Quantity limits determine whether the labeled induction or maintenance plan can be filled without exception. Renewal criteria determine whether a patient stays on therapy after the first approval period.
A useful matrix separates initial approval from renewal. Initial criteria might require diagnosis code, baseline severity, biomarker status, contraindication to preferred agents, or specialist attestation. Renewal criteria might require response documentation, adherence, lab monitoring, or absence of safety issues. Those are different operational tasks.
Add specialty-pharmacy routing
Specialty pharmacy is not a footnote. Limited-distribution networks, plan-mandated specialty pharmacies, white-bagging rules, and hub routing can make a covered drug functionally unavailable. The matrix should show which specialty pharmacies are required, whether the manufacturer hub can transfer prescriptions, and where benefit investigation is performed.
This is also where patient-support operations meet payer policy. A perfect copay program is useless if the patient is routed to a non-participating pharmacy. A PAP can be delayed if benefit investigation fails to capture denial documentation. The access page should make those dependencies visible.
PAP and copay logic belong in the same view
Patient assistance and copay support are usually described separately from coverage. In practice they are triggered by coverage. Commercially insured patients may need copay support. Medicare and Medicaid patients face different legal and program constraints. Uninsured or underinsured patients may need PAP eligibility screening. A patient who is denied coverage may need appeal support before PAP eligibility is clear.
The matrix should include:
- commercial copay program availability;
- government-insurance exclusions;
- PAP income thresholds if disclosed;
- required denial or benefit-investigation documentation;
- renewal cadence;
- bridge or quick-start program limits;
- appeal-support pathway.
This turns access content from a marketing module into a workflow.
Build around source documents
The strongest source set is not one page. It is a combination of payer medical policies, plan formularies, CMS materials for Medicare context, FDA labels for indication limits, DailyMed for current prescribing information, and manufacturer support-program pages for eligibility details. When payer policies differ, the matrix should show difference rather than flattening it into a national claim.
That is the differentiation opportunity in R68/R68b. GoodRx can win coupon queries. Manufacturer pages can win brand navigation. PharmaDossier can win the structured layer: the thing a market-access team wishes every search result already showed.
Sources
- DailyMed drug label database: https://dailymed.nlm.nih.gov/dailymed/
- CMS Medicare Coverage Center: https://www.cms.gov/medicare-coverage-database/
- CMS Prescription Drug Coverage: https://www.cms.gov/medicare/prescription-drug-coverage
- FDA Drugs@FDA database: https://www.accessdata.fda.gov/scripts/cder/daf/