A manufacturing site change for a commercial biologic ordinarily requires a Prior Approval Supplement (PAS) under 21 CFR 601.12(b), with FDA review clocks that can run four months or longer. For launch teams managing supply continuity, that timeline is a choke point: every week the new site is not approved is a week the product is unavailable from that facility. A Post-Approval Change Management Protocol (PACMP), which FDA refers to as a Comparability Protocol (CP) in its October 2022 final guidance, offers a regulatory tool to prospectively negotiate a reduced reporting category, shortening the clock to as little as 30 days or even an annual report for some changes.
This article is for regulatory affairs leads, CMC strategy directors, and manufacturing directors planning a site transfer for an approved biologic. It covers when a PACMP is the right tool, how to build one for a site change, and where the common failure points are.
When a PACMP fits a site change
The reporting-category spectrum
Under 21 CFR 601.12, post-approval changes to biologics follow a tiered reporting structure:
| Reporting category | Typical review clock | Distribution constraint |
|---|---|---|
| Prior Approval Supplement (PAS) | 4 months (standard); 6 months for complex reviews | Cannot distribute until FDA approves |
| Changes Being Effected in 30 Days (CBE-30) | 30 days | Can distribute after 30 days if no FDA action |
| Changes Being Effected (CBE-0) | 0 days | Can distribute upon submission |
| Annual Report | None | Can distribute immediately |
A PACMP does not change the underlying regulation. Instead, it lets a sponsor prospectively negotiate a lower reporting category by agreeing to a defined set of studies and acceptance criteria that FDA reviews and approves in advance. When the sponsor later executes the studies and meets the criteria, the implementation step is filed at the agreed-upon lower category.
FDA's 2022 Comparability Protocol guidance
FDA's final guidance, Comparability Protocols for Postapproval Changes to the Chemistry, Manufacturing, and Controls Information in an NDA, ANDA, or BLA (October 2022, FDA-2016-D-0973), establishes that a CP/PACMP is a "comprehensive, prospectively written plan for assessing the effect of a proposed postapproval CMC change(s) on the identity, strength, quality, purity, and potency of a drug product, including a biological product."
The guidance confirms that a CP may be submitted in an original BLA or subsequently as a stand-alone PAS. Once FDA approves the protocol, the sponsor may implement the change at the reduced reporting category, provided the acceptance criteria are met.
Site changes: the constraint FDA flags
The 2022 guidance includes an important limitation: "Future manufacturing site changes or certain other changes that may require a facility evaluation proposed in a CP generally do not justify a reporting category other than a PAS or CBE-30." The reason is that FDA needs to evaluate whether the proposed facility requires a pre-approval inspection at the time the change is implemented, and that assessment cannot be done at the time the CP is submitted if the facility is not yet known or may change in compliance status.
This means that for biologic site changes, the best-case outcome from a PACMP is typically a reduction from PAS to CBE-30, not to annual report. Even that reduction saves the sponsor three months of review clock per site addition.
ICH Q12 and the two-step PACMP structure
Step 1: Protocol submission and FDA review
Under ICH Q12, a PACMP follows a two-step process. In Step 1, the sponsor submits the protocol as a written plan. The protocol must include:
- Description of the proposed change: The specific site change, including the product, the current site, the proposed site, and the manufacturing operations to be transferred.
- Risk assessment: An evaluation of the potential impact on product quality, including CQAs, process parameters, and the control strategy.
- Studies and acceptance criteria: The comparability studies, analytical tests, process-validation activities, and stability program the sponsor will execute, with predefined acceptance criteria for each.
- Proposed reporting category: The reduced reporting category the sponsor is requesting for Step 2 implementation.
- Conditions for implementation: Any prerequisites, such as successful process validation, satisfactory inspection history at the proposed site, or completion of a technology transfer.
FDA reviews the protocol as part of a PAS submission. The review clock runs like any PAS, typically four months. At the end of Step 1, FDA either approves the protocol as proposed, approves it with modifications, or issues a complete response.
Step 2: Protocol execution and implementation
After the protocol is approved, the sponsor executes the agreed-upon studies at the new site. When the results meet the acceptance criteria, the sponsor submits the results at the agreed-upon reporting category (e.g., CBE-30). FDA reviews the submission within the shorter clock, and the sponsor can distribute product from the new site.
If the results do not meet the acceptance criteria, the change cannot be implemented under the PACMP. The sponsor must either submit a standard PAS with full justification or revise the protocol and start over.
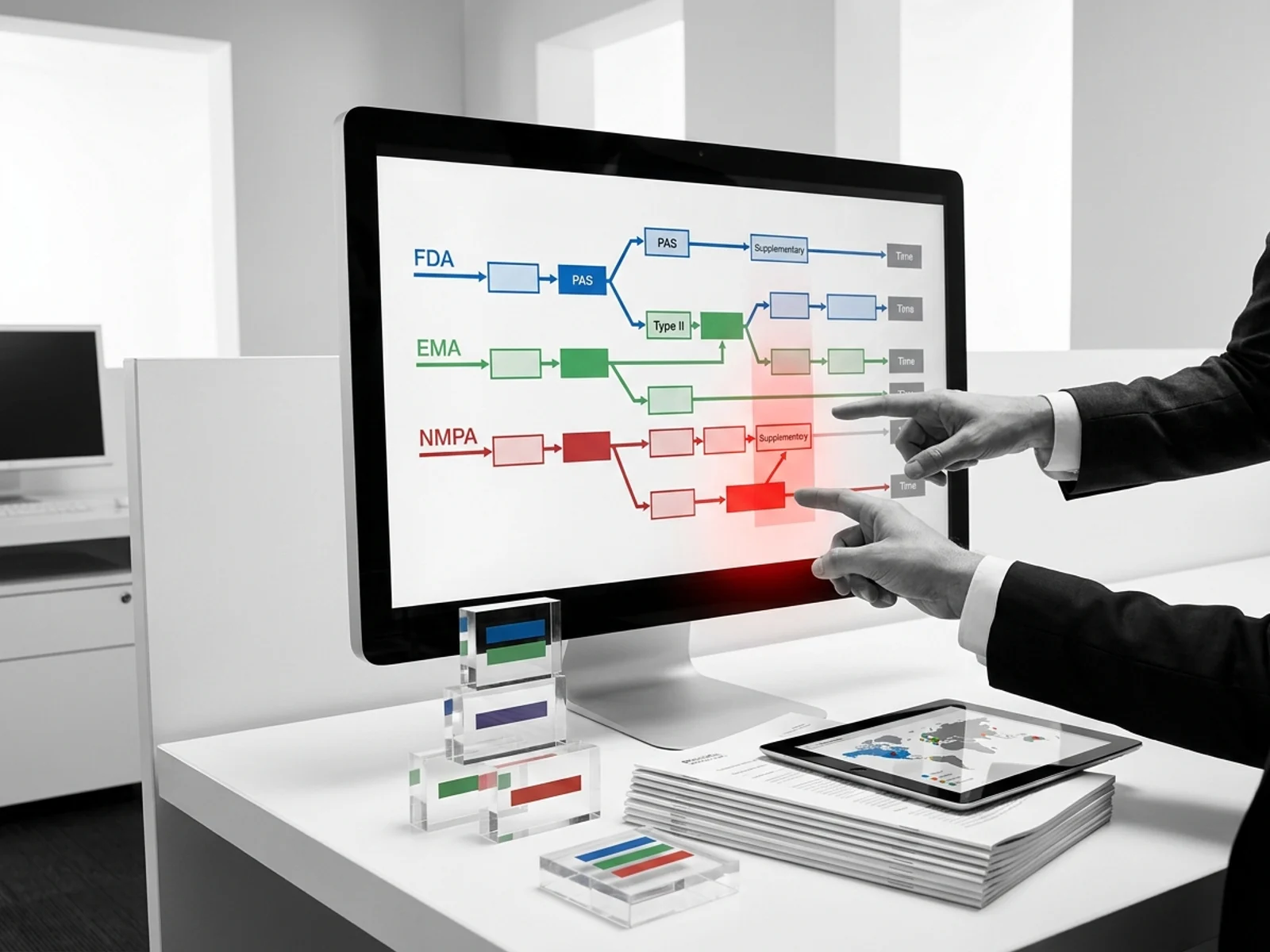
The Novo Nordisk case study
At the October 2024 CASSS CMC Strategy Forum, Novo Nordisk presented three PACMP case studies. In Case III, the company added drug product formulation and filling sites using a reusable PACMP. The outcome: for FDA, the reporting category dropped from PAS to CBE-30. For EMA, the category dropped from Type II variation to Type IB. For Swissmedic, the same reduction applied. The company reported that the prior agreement from Step 1 enabled faster implementation across multiple markets.
This case demonstrates that the PACMP framework works in practice for site additions, but the achievable reduction is typically one tier (PAS to CBE-30), not two tiers (PAS to annual report).
Building the protocol: what must be in the submission
Comparability bridge
The core of any biologic site-change PACMP is the comparability bridge. FDA's 2022 guidance and ICH Q5E require the sponsor to demonstrate that the product manufactured at the new site is comparable to the product manufactured at the existing site in terms of identity, strength, quality, purity, and potency. For a complex biologic, this typically requires:
- Side-by-side analytical characterization (glycosylation, charge variants, size variants, biological activity)
- Process validation at the new site (minimum three consecutive batches at commercial scale)
- Accelerated and long-term stability studies at protocol-defined time points
- Nonclinical pharmacokinetic bridging studies, if warranted by the risk assessment
Acceptance criteria design
The acceptance criteria in the PACMP must be predefined and objective. The 2022 guidance states: "The acceptance criteria for the change can allow for differences in product attributes if you provide justification based on your assessment of the effect(s) of the change on safety and effectiveness. If you anticipate such differences, they should be prospectively described."
For a site change, acceptance criteria typically include:
| Attribute | Typical acceptance approach |
|---|---|
| Identity | Confirmatory assay matches reference standard |
| Purity/impurity profile | Within established trending limits; no new impurity species |
| Potency | Within release specification range |
| Glycosylation (for mAbs) | Predefined similarity criteria for major glycoforms |
| Process parameters | All critical process parameters within validated ranges |
| Stability | No statistically significant difference from reference at protocol time points |
Process validation requirements
FDA expects that process validation at the new site will be completed before the Step 2 submission. The protocol should specify the number of validation batches (typically three consecutive at commercial scale), the in-process controls to be monitored, and the acceptance criteria for each unit operation. If process validation fails, the sponsor cannot proceed with Step 2.
Stability program
The PACMP should define the stability protocol for product manufactured at the new site, including the number of batches to be placed on stability, the storage conditions, the testing time points, and the criteria for confirming comparable stability profiles. FDA typically expects at least six months of accelerated and long-term stability data at the time of Step 2 submission for a site change, though the protocol may allow initial distribution with commitment to ongoing stability monitoring.
Common failure points
Failure 1: Vague or open-ended acceptance criteria
FDA will not approve a PACMP that uses subjective language such as "comparable," "similar," or "no significant difference" without predefined quantitative criteria. The 2022 guidance is explicit: acceptance criteria must be specific and measurable. Sponsors who submit protocols with open-ended criteria receive complete response letters requesting revision.
Failure 2: Insufficient risk assessment
The risk assessment must identify every potential impact pathway from the site change to product quality. For biologics, this includes immunogenicity risk from process changes that could affect product-related variants. A risk assessment that merely states "low risk" without supporting data will not support a reduced reporting category.
Failure 3: Cumulative drift from reusable PACMPs
FDA's guidance warns that for changes made repeatedly under the same PACMP, the sponsor must design the protocol to ensure that "the effects of such cumulative changes will not result in an unintentional drift in product quality over time." Each execution of the protocol should include trending analysis against the original reference product data, not just against the most recent batch.
Failure 4: Facility compliance status changes between Step 1 and Step 2
If the proposed facility's CGMP compliance status deteriorates between the time the protocol is approved and the time it is executed, FDA may require a PAS instead of the agreed-upon CBE-30. Sponsors should monitor the inspection history of the target facility continuously and have contingency plans for alternative sites.
Failure 5: Scope creep beyond CMC-only changes
A PACMP is suitable only for CMC changes. If the site change also requires clinical data, efficacy supplements, or labeling changes, the PACMP cannot cover those elements. Sponsors must file those changes separately through the appropriate regulatory pathway.
Strategic considerations for launch teams
Timing: when to file the PACMP
The optimal time to file a PACMP for a planned site change is 12 to 18 months before the sponsor intends to distribute product from the new site. The Step 1 review takes approximately four months. Technology transfer and process validation take six to twelve months. Step 2 review under CBE-30 adds 30 days. Sponsors who wait until the site is ready and then file a standard PAS face the full four-month review clock without the benefit of prior agreement.
Multi-product PACMPs
FDA's 2022 guidance and ICH Q12 both support the use of PACMPs across multiple products or multiple BLAs (a "trans-BLA" protocol). For a sponsor transferring an entire manufacturing platform to a new site, a single PACMP can cover multiple products, reducing the number of separate filings and consolidating the comparability evidence.
Global alignment: EMA and non-ICH markets
The IFPMA 2024 global survey of post-approval change frameworks found that 59% of markets include grace periods for implementation of CMC post-approval changes. The EU's draft variation guidelines (2025) provide for PACMPs, extrapolation, modeling approaches, and acceptance of pilot-scale batches for certain variations. However, classification of the same site change may differ across markets. The same change that is CBE-30 at FDA may be Type IB at EMA and a notification in a non-ICH market. Sponsors should build global variation strategy into the PACMP from the start.
Sources
- FDA. Comparability Protocols for Postapproval Changes to the Chemistry, Manufacturing, and Controls Information in an NDA, ANDA, or BLA. October 2022. https://www.fda.gov/media/162263/download
- FDA. ICH Q12: What Industry Needs to Know. https://www.fda.gov/media/174238/download
- FDA. Certain Biological Products; Guidance for Industry. https://www.fda.gov/media/109615/download
- ICH. Q12 Technical and Regulatory Considerations for Pharmaceutical Product Lifecycle Management. November 2019. https://database.ich.org/sites/default/files/ICH_Q12_Guideline_Step4_2019_1119.pdf
- EFPIA. Post-Approval Change Management Protocols (PACMPs) Reference Document. https://www.efpia.eu/media/554680/post-approval-change-management-protocols-pacmps-reference-document.pdf
- IFPMA. Global Regulatory Approaches to Post-Approval Changes in Biotherapeutic Products. December 2024. https://www.ifpma.org/wp-content/uploads/2024/12/1025_Global-regulatory-approaches-to-post-approval-changes-in-biotherapeutic-products_Clarivate_IFPMA.pdf
- Federal Register. Comparability Protocols for Postapproval Changes. October 14, 2022. https://www.federalregister.gov/documents/2022/10/14/2022-22334
- Basu Sen S. Industry Perspective on the Use of Post-Approval Change Management Protocols. CASSS CMC Strategy Forum Europe. October 2024. https://www.casss.org/docs/default-source/cmc-strategy-forum-europe/2024-speaker-presentations/basu-sen-shrobona-novo-nordisk-a-s-2024.pdf