When the Inflation Reduction Act required every Medicare Part D plan to cover drugs selected for the Medicare Drug Price Negotiation Program, it also built in an escape hatch: plans may remove a selected drug from formulary when a generic or biosimilar competitor arrives. The mechanism is the "successor regulation" exception, and its operational details — finalized by CMS in the CY 2026 Part D Redesign Program Instructions — determine whether a branded selected drug keeps its guaranteed formulary slot or gets displaced by a lower-cost competitor within weeks of launch.
For manufacturer launch teams, payer strategy groups, and formulary designers, the successor regulation exception is not a footnote. It is the structural rule that determines whether an MFP remains commercially relevant after generic or biosimilar entry, and how quickly Part D plan sponsors can redesign formularies to capture cost savings.
The statutory formulary inclusion requirement
Section 1860D-4(b)(3)(I)(i) of the Social Security Act, added by section 11001(b) of the IRA, requires that starting in 2026, Part D plan sponsors include on their formularies every covered Part D drug that is a "selected drug" for which a maximum fair price is in effect. This is a departure from standard Part D formulary practice, where plan sponsors have broad discretion to exclude drugs, place them on non-preferred tiers, or apply utilization management — subject only to CMS formulary review and protected-class requirements.
The formulary inclusion requirement means that when CMS negotiated MFPs for the first 10 selected drugs taking effect January 1, 2026, every Part D plan — standalone PDPs and Medicare Advantage-Prescription Drug (MA-PD) plans — had to add these drugs to formulary. Avalere Health's analysis of the 2026 Part D formulary files found that this requirement drove significant coverage expansion. Farxiga, which had been covered on 76% of formularies in 2025, moved to near-universal coverage. Stelara and Entresto, which had more limited Part D formulary presence, became required on all plans.
But the statute also included section 1860D-4(b)(3)(I)(ii): nothing in the inclusion requirement prohibits plans from removing a selected drug "if such removal would be permitted under § 423.120(b)(5)(iv) or any successor regulation."
The successor regulation puzzle
At the time the IRA was enacted in August 2022, § 423.120(b)(5)(iv) of the CMS regulations permitted a plan to immediately substitute a newly available generic drug for its brand-name drug on formulary, subject to notice and timing requirements. But the CY 2025 Parts C & D Final Rule reorganized and renumbered the Part D formulary regulations, and § 423.120(b)(5)(iv) ceased to exist in its original form.
CMS therefore had to identify the "successor regulation" — the current regulatory provision that carries forward the same immediate-substitution authority. In the Final CY 2026 Part D Redesign Program Instructions, published April 7, 2025, CMS finalized its identification of the successor regulation as the combination of:
- § 423.120(e)(2)(i), which governs the approval requirements for immediate formulary substitutions; and
- § 423.120(f)(2), (3), and (4), which govern the notice requirements for such formulary changes.
This identification was not uncontroversial. Several commenters on the draft CY 2026 program instructions argued that the original § 423.120(b)(5)(iv) was specific to generic drug substitutions and that CMS lacked authority to extend the successor regulation exception to biosimilar biological products. CMS disagreed, finalizing the position that the current regulatory framework — which covers both generic and biosimilar immediate substitutions — constitutes the successor regulation.
How the 30-day formulary window works
Under the finalized successor regulation exception, when a generic drug or biosimilar biological product launches for a selected drug, Part D plan sponsors have a 30-day window to remove the selected drug from formulary, provided they add the corresponding generic or biosimilar at an equal or better tier placement.
The CY 2026 program instructions bifurcate plan options depending on whether the corresponding drug launches before or after initial formulary submissions in June:
- If the generic or biosimilar launches before the June formulary reference file (FRF) submission: Plans can include the generic or biosimilar on their initial formulary submission and may remove the selected drug at that time, subject to the equal-or-better-tier requirement.
- If the generic or biosimilar launches after the June FRF submission: Plans have a 30-day window from the date the corresponding drug becomes available to make a mid-year formulary change, removing the selected drug and adding the generic or biosimilar.
This timing matters because several 2026 selected drugs face imminent generic or biosimilar entry. Milliman's analysis identified key entrants:
| Selected Drug | Generic/Biosimilar | Expected Launch | MFP Drug in 2026? |
|---|---|---|---|
| Farxiga | dapagliflozin | 2025–2026 | Yes |
| Entresto | sacubitril/valsartan | 2025 | Yes (removed 2027) |
| Xarelto | rivaroxaban | 2025 | Yes (removed 2027) |
| Stelara | ustekinumab biosimilars | 2025 | Yes (removed 2027) |
| Januvia | sitagliptin | 2026 | Yes |
What happens to the MFP when generics arrive
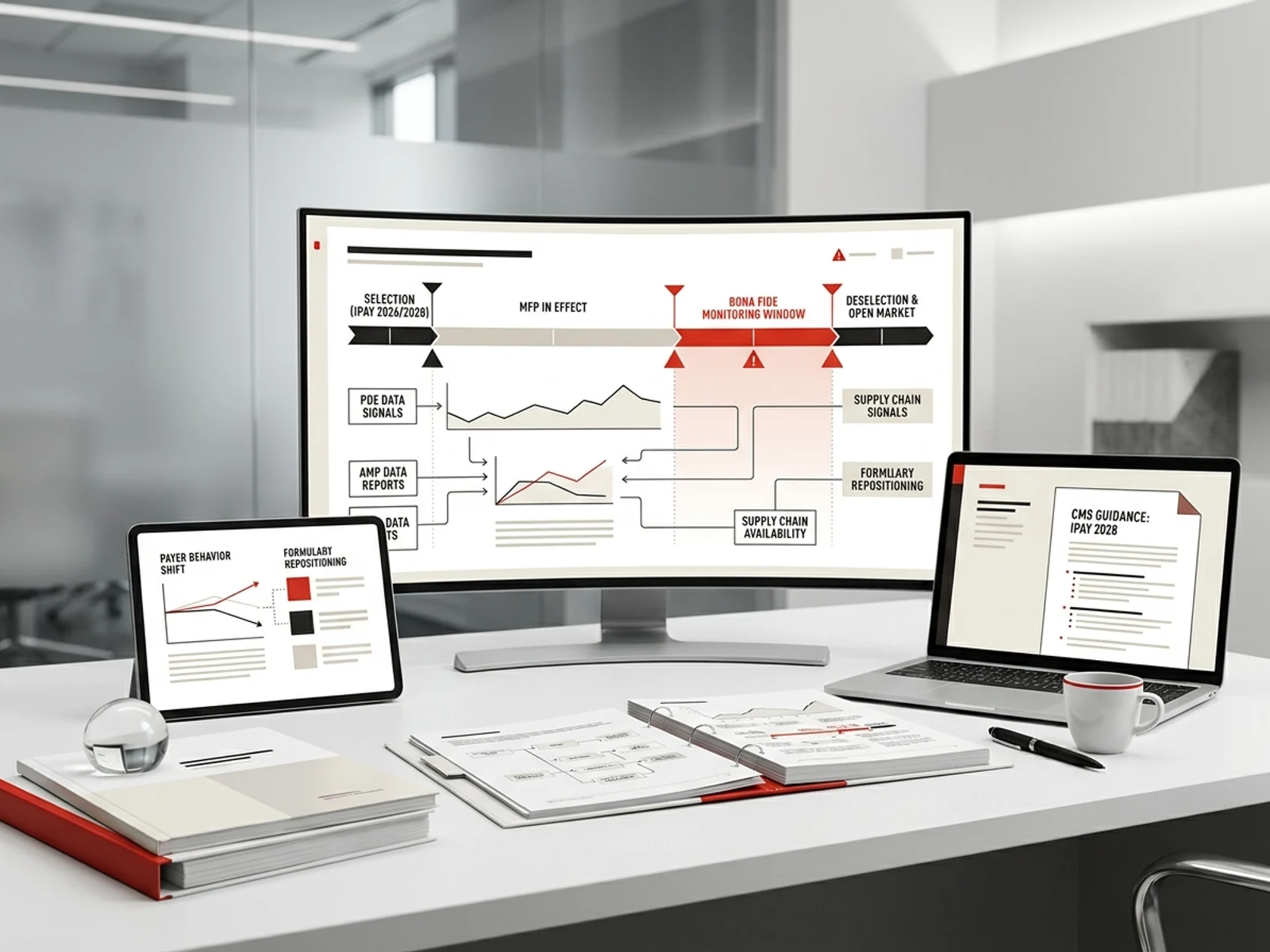
The interaction between the successor regulation exception and the MFP itself is critical. CMS has confirmed that the MFP remains in effect as long as the drug is a selected drug, even if a generic or biosimilar launches. The MFP does not vanish the moment a competitor enters the market. Instead, CMS must make a "bona fide marketing" determination — a finding that the generic or biosimilar is not just approved but is actively and consistently available in the market.
CMS uses a "totality of the circumstances" inquiry for bona fide marketing determinations. Sources include:
- Prescription Drug Event (PDE) data showing claims for the generic or biosimilar;
- Average Manufacturer Price (AMP) data reported by generic or biosimilar manufacturers;
- Whether the product is regularly and consistently available through the pharmaceutical supply chain;
- Whether any licensing agreements between the primary manufacturer and the generic or biosimilar manufacturer limit availability.
CMS announced in late 2025 that Entresto, Stelara, and Xarelto would be removed from the selected drug list effective January 1, 2027, after determining that at least one approved generic or biosimilar version of each drug was being bona fide marketed. This means:
- For 2026, these three drugs still have MFPs and must be on every Part D formulary.
- Starting January 1, 2027, the MFPs no longer apply, and plans are free to remove these drugs and substitute generics or biosimilars — subject to the successor regulation's equal-or-better-tier requirement.
The removal of these three drugs from MFP applicability has financial significance. HHS projected that MFPs would produce approximately $6 billion in reduced Medicare program spending for the 2026 selected drugs, plus $1.5 billion in out-of-pocket cost savings for beneficiaries. Entresto, Stelara, and Xarelto — drugs that will lose their MFPs after just one year — account for a significant share of that first-year savings.
Authorized generics do not trigger the exception
A critical distinction for launch teams: the IRA specifies that authorized generics do not count as generic drugs for purposes of negotiation eligibility or the formulary inclusion exception. An authorized generic is the same drug product as the brand-name drug with a different label — manufactured by or under license from the primary manufacturer. Because authorized generics are not independent competitors, their availability does not trigger:
- Disqualification from negotiation eligibility;
- Removal from the selected drug list; or
- The successor regulation formulary substitution exception.
This means a manufacturer that launches an authorized generic alongside its branded selected drug retains the formulary inclusion requirement and the MFP — the authorized generic does not give plans a pathway to remove the branded product from formulary under the successor regulation.
What this means for launch and lifecycle teams
The successor regulation exception creates several actionable planning points:
For manufacturers of selected drugs facing generic or biosimilar entry: Model the 30-day formulary window into revenue forecasts. Once a generic or biosimilar launches and CMS confirms bona fide marketing, plans can shift formulary positioning rapidly. The guaranteed formulary slot that the MFP provides has a finite — and potentially short — commercial life.
For manufacturers of therapeutic alternatives to selected drugs: The formulary inclusion requirement can work in your favor when a selected drug's MFP makes it competitively priced. But when the MFP disappears (as with Entresto, Stelara, and Xarelto in 2027), plans regain full formulary discretion. Model the post-MFP competitive landscape separately from the MFP-in-effect period.
For Part D plan sponsors: The successor regulation exception gives a clear operational pathway: when a generic or biosimilar launches, you have 30 days to execute a formulary substitution that places the competitor at an equal or better tier. Track CMS bona fide marketing determinations — they determine when the MFP stops applying and when the formulary landscape opens up.
For 2028 and beyond: The 2028 negotiation cycle includes 15 Part B and Part D drugs, several of which face anticipated generic or biosimilar competition before or during the negotiation period. Milliman noted that Xeljanz and Xolair, both selected for IPAY 2028, are expected to face generic and biosimilar competition respectively in 2026, and CMS may never announce MFPs for these drugs if bona fide marketing is confirmed before the November 2026 negotiation deadline. Trulicity, another 2028 selection, faces anticipated biosimilar entry in 2027, which could result in removal after just one year of MFP applicability.
Sources
- CMS, "Final CY 2026 Part D Redesign Program Instructions," April 7, 2025. https://www.cms.gov/files/document/final-cy-2026-part-d-redesign-program-instruction.pdf
- CMS, "Final CY 2026 Part D Redesign Program Instructions Fact Sheet." https://www.cms.gov/newsroom/fact-sheets/final-cy-2026-part-d-redesign-program-instructions
- KFF, "Key Facts About Medicare Drug Price Negotiation," updated 2026. https://www.kff.org/medicare/key-facts-about-medicare-drug-price-negotiation
- Milliman, "Prescribing a Part D formulary for the new IRA world." https://www.milliman.com/en/insight/prescribing-part-d-formulary-new-ira
- Milliman, "Medicare drug price negotiation: New dynamics as the tide turns to Part B." https://www.milliman.com/en/insight/medicare-drug-price-negotiation-part-b-dynamics
- HHS, "Medicare Drug Price Negotiation Program: Negotiated Prices for Initial Price Applicability Year 2026." https://www.cms.gov/newsroom/fact-sheets/medicare-drug-price-negotiation-program-negotiated-prices-initial-price-applicability-year-2026
- DLA Piper, "Evaluating biologic drug costs: Medicare negotiated prices versus biosimilar competition," March 2026. https://www.dlapiper.com/insights/publications/2026/03/evaluating-biologic-drug-costs
- NCPA, "Entresto, Stelara and Xarelto will exit the Medicare Drug Price Negotiation Program beginning Jan. 1, 2027," December 2, 2025. https://ncpa.org/newsroom/qam/2025/12/02/entresto-stelara-and-xarelto-will-exit-medicare-drug-price-negotiation
- Avalere Health, "Part D Formulary Management Tightens in 2026." https://advisory.avalerehealth.com/insights/part-d-formulary-management-tightens-in-2026
- Applied Policy, "For 2026, CMS Finalizes Changes Resulting in a 5.06 Percent…" https://www.appliedpolicy.com/wp-content/uploads/CY-2026-MA-and-Part-D-Rate-Announcement-and-Part-D-Redesign-Program-Instructions-4.7.25.pdf