A GLP-1 benefit investigation is the foundational step before any prior authorization submission, specialty pharmacy routing, or patient assistance enrollment. It answers four questions: Is the drug on formulary? Does it require PA? Which specialty pharmacy does the plan mandate? What will the patient pay? Skipping or shortcutting the benefit investigation is the single most common reason GLP-1 prescriptions stall at the pharmacy counter.
This guide provides a step-by-step GLP-1 benefit investigation workflow, maps what to look for on formulary documents and payer portals, details what to ask during the benefits verification call, and explains how to interpret the outcomes. It is independent information and not medical advice or reimbursement guidance for a specific patient or plan.
Quick answer
| Investigation Step | What to Find | Where to Look |
|---|---|---|
| Formulary status | Is the GLP-1 on formulary? Preferred or non-preferred? Which tier? | Payer formulary document, PBM website, ePA platform |
| PA requirement | Is prior authorization required? What are the clinical criteria? | Payer PA criteria document, clinical policy bulletin |
| Step therapy | Does the plan require trying another drug first? Which one? | Formulary notes, PA criteria document |
| Specialty pharmacy routing | Is the patient locked to a specific specialty pharmacy? Which one? | Payer specialty pharmacy list, PBM network directory |
| Patient cost share | What is the copay, coinsurance, or deductible amount? | Plan benefit document, pharmacy benefit desk call |
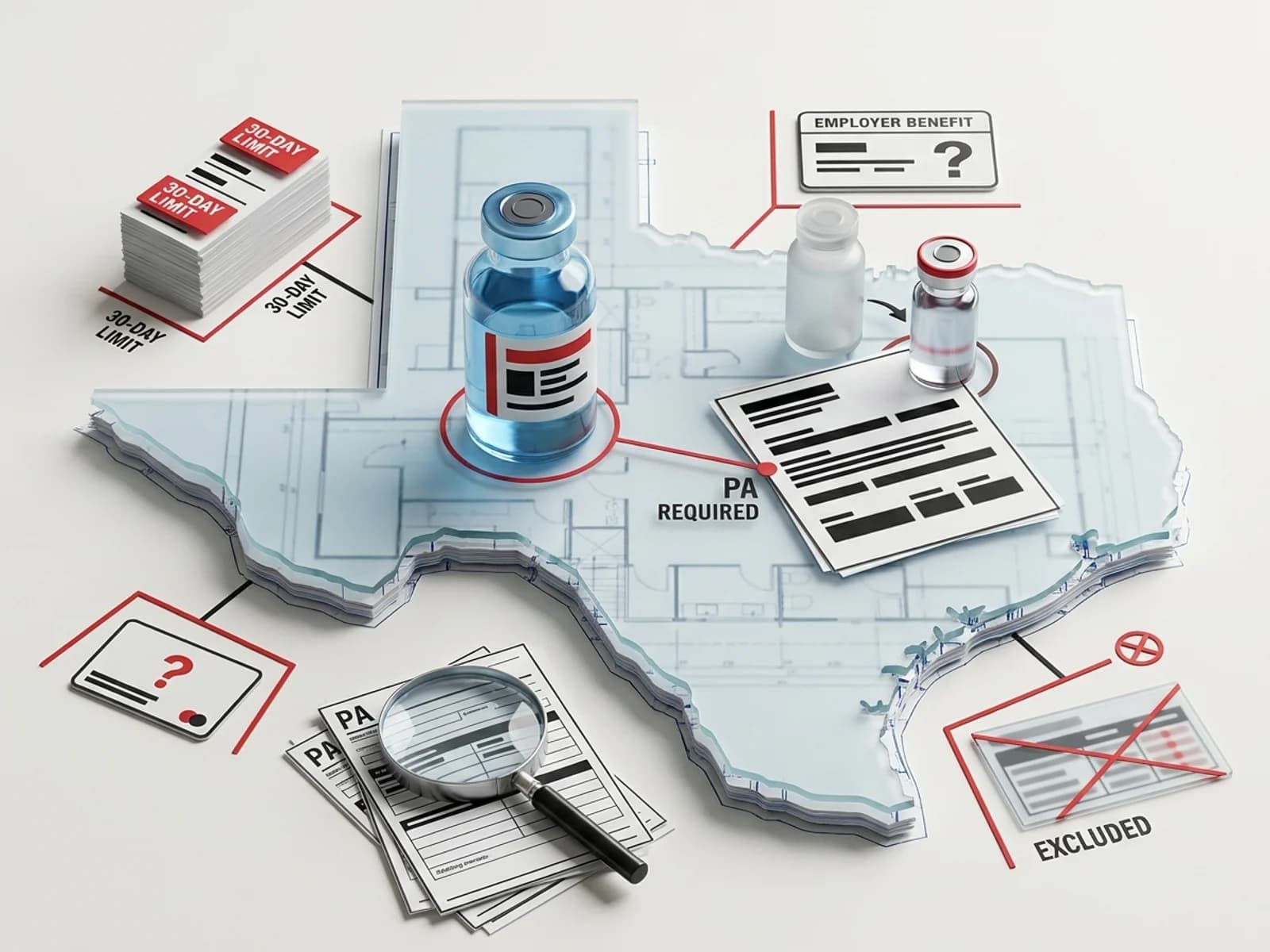
| Quantity limits | Is there a dose or quantity limit? 30-day supply only? | Formulary notes, PA criteria document |
| Benefit exclusion | Is weight loss / obesity treatment excluded from the plan benefit entirely? | Plan benefit summary, employer benefit election verification |
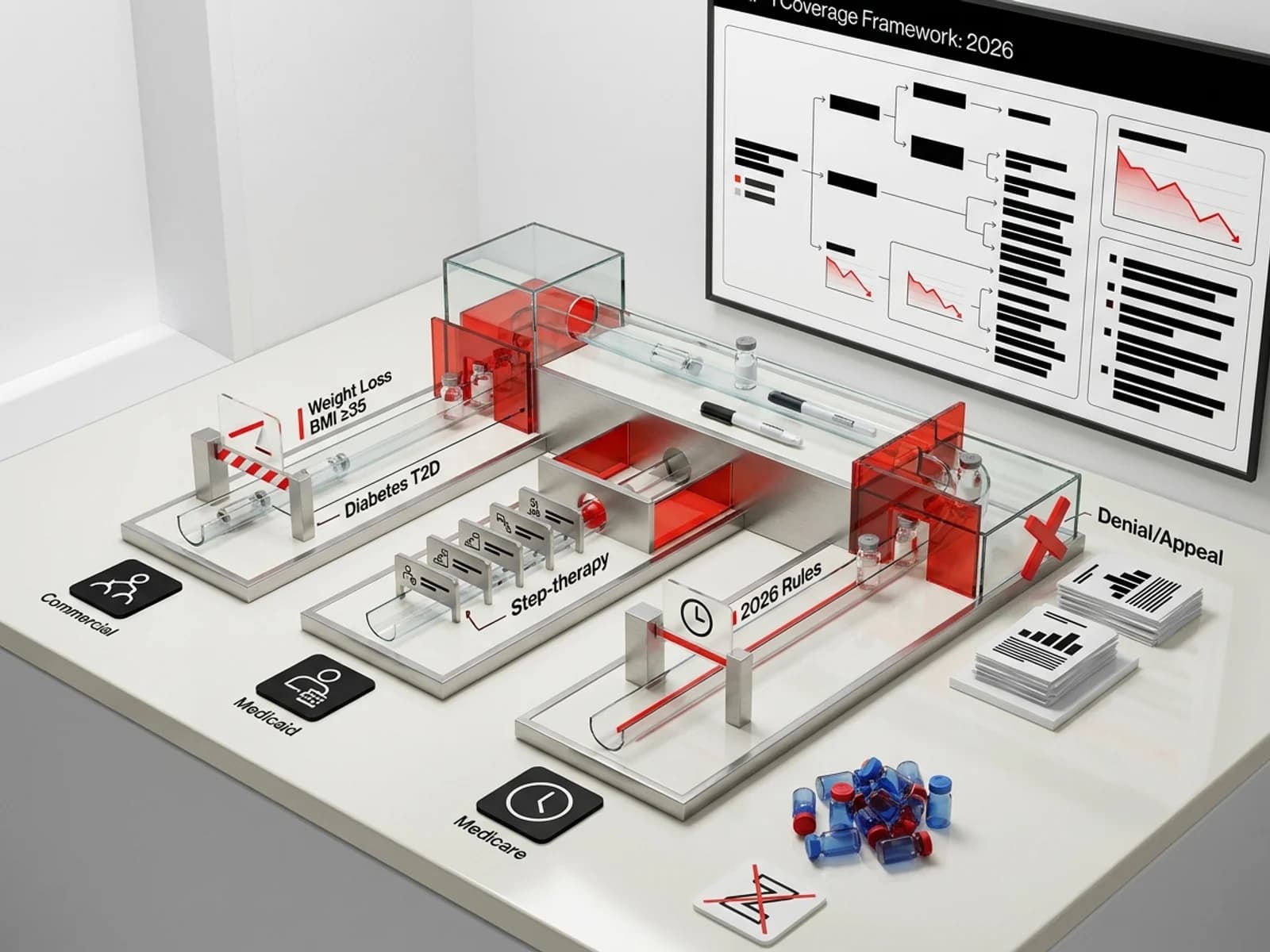
Key context for 2026:
- 43% of firms with 5,000+ employees now cover GLP-1s for weight loss, up from 28% in 2024 (KFF/Health Affairs survey)
- 57% of employers overall cover GLP-1s for weight loss (WTW survey data)
- 13 state Medicaid programs cover GLP-1s for obesity as of January 2026, down from 16 in 2025 (KFF)
- Multiple payers (Blue Cross of Massachusetts, VEHI, Independent Health) have implemented benefit exclusions for GLP-1 weight-loss drugs effective January 1, 2026
Who this is for
- Prescribers and clinic staff verifying GLP-1 benefits before writing prescriptions
- Benefit verification specialists and hub support teams conducting GLP-1 benefit investigations
- Pharmacists navigating GLP-1 prior authorization and specialty pharmacy routing
- Market access teams tracking payer coverage trends for GLP-1 formulary positioning
- Patients trying to understand whether their plan covers a specific GLP-1 medication
Source standard
Every fact in this guide is sourced from payer formulary documents, clinical policy bulletins, CMS regulatory publications, manufacturer hub program materials (Novo Nordisk NovoCare, LillyDirect), KFF analyses, industry reports from IntuitionLabs, Truveris, and Mercer dated 2025–2026. Benefit details vary by plan, state, and employer election. Always verify current coverage by calling the member services number on the patient's insurance card or checking the payer's provider portal.
The GLP-1 benefit investigation workflow
Step 1: Confirm the patient's plan information
Before investigating, confirm:
- Payer name (e.g., UnitedHealthcare, Aetna, BCBS of Texas)
- Plan type (commercial, Medicaid, Medicare Advantage, ACA marketplace)
- Plan ID / group number (from the insurance card)
- Pharmacy benefit manager (may differ from the medical payer — e.g., UHC medical with OptumRx pharmacy)
- Whether the plan is self-funded or fully insured (self-funded employers choose their own GLP-1 benefit design; fully insured plans follow the payer's standard formulary)
Self-funded plans are a critical variable. A patient insured through "Cigna" may have a self-funded employer plan that excludes all weight-loss GLP-1s, while another Cigna patient at a different employer has full coverage. The benefit investigation must identify whether the employer has purchased a GLP-1 rider or excluded GLP-1 weight-loss drugs entirely.
Step 2: Check formulary status
Look up the specific GLP-1 drug on the plan's formulary:
Where to check:
- Payer's provider portal formulary search (e.g., UHCprovider.com, Aetna provider portal)
- PBM website formulary tool (e.g., CVS Caremark, Express Scripts, OptumRx)
- Electronic formulary tools: Surescripts On-Demand Formulary, CoverMyMeds formulary check, EHR-integrated formulary lookup
- Novo Nordisk's NovoCare formulary finder for Wegovy and Ozempic
- Eli Lilly's LillyDirect coverage check for Mounjaro and Zepbound
What to look for:
| Formulary Status | What It Means | Next Step |
|---|---|---|
| On formulary, Tier 2–3 (preferred) | Covered with standard PA; lowest cost share | Proceed to PA check |
| On formulary, Tier 3–4 (non-preferred / specialty) | Covered but higher cost share; may require step therapy | Check step therapy requirements |
| Not on formulary | Drug is excluded from the plan's covered drug list | Request formulary exception or check alternative GLP-1 |
| Benefit excluded (not just non-formulary) | The plan does not cover GLP-1s for the requested indication at all | Verify if any GLP-1 is covered for other indications (e.g., T2D, MACE risk reduction) |
Critical distinction — non-formulary vs. benefit exclusion: A non-formulary drug can still be obtained through a formulary exception with PA. A benefit exclusion means the plan does not cover GLP-1s for the specified indication under any circumstances. Blue Cross of Massachusetts, for example, implemented a benefit exclusion for GLP-1s used for obesity effective January 1, 2026, with no exceptions process — unless the member's employer purchased a rider.
Step 3: Check prior authorization requirements
If the GLP-1 is on formulary (or may qualify for a formulary exception), check PA requirements:
Where to check:
- Payer's clinical policy bulletins (e.g., Aetna Clinical Policy Bulletins, UHC pharmacy clinical guidelines)
- Payer's PA criteria documents (often in PDF format on the provider portal)
- CoverMyMeds or Surescripts ePA platform (shows PA requirements and criteria at the point of prescribing)
What to document:
- Is PA required for this specific GLP-1 on this specific plan?
- What are the clinical criteria? (BMI threshold, comorbidity requirements, lifestyle program documentation, prior-therapy requirements)
- Is there a specific PA form, or can a general PA form be used?
- What is the fax number or electronic submission pathway?
- What is the expected turnaround time? (72 hours expedited / 7 days standard under CMS-0057-F for Medicare Advantage and Medicaid; commercial timelines vary)
Step 4: Identify specialty pharmacy requirements
Most GLP-1 prescriptions are routed through specialty pharmacy channels. The benefit investigation must determine:
Mandatory specialty pharmacy:
Many plans require GLP-1 prescriptions to be filled through a specific specialty pharmacy:
- Accredo (Express Scripts / Cigna): Mandatory for many Cigna and Express Scripts plans
- CVS Specialty: Mandatory for many Aetna and CVS Caremark plans
- Optum Specialty Pharmacy: Mandatory for many UHC / OptumRx plans
- AllianceRx Walgreens Prime: Mandatory for some BCBS plans using Prime Therapeutics
- Limited distribution drugs (LDD): Some GLP-1 formulations are available only through specific pharmacies contracted with the manufacturer. If the plan designates the drug as an LDD, the patient must use the designated specialty pharmacy — no exceptions.
What happens if you send the prescription to the wrong pharmacy:
The prescription will be rejected at point of sale with a "pharmacy not in network" or "must use designated specialty pharmacy" rejection code. The patient cannot simply take the prescription to their preferred retail pharmacy if the plan mandates specialty pharmacy dispensing.
Step 5: Verify patient cost share
Determine what the patient will pay:
Questions for the benefits verification call:
- What is the copay or coinsurance for this drug under the patient's plan?
- Is the drug subject to the deductible? If so, how much of the deductible has been met?
- Is there a copay card or manufacturer savings program that can be applied?
- Is the plan using a copay accumulator or maximizer program? (If yes, manufacturer copay cards may not count toward the patient's deductible or out-of-pocket maximum.)
Manufacturer savings and self-pay programs (2026):
- Wegovy copay card (commercial insurance, Novo Nordisk): As low as $25/month for eligible commercially insured patients, subject to a maximum savings of $100/month. Government beneficiaries excluded.
- Wegovy self-pay pricing (NovoCare Pharmacy): $149/month for Wegovy tablets (1.5 mg and 4 mg); $199/month for first 2 months of injections (starter doses 0.25 mg and 0.5 mg) through June 30, 2026, then $349/month for standard injections and $399/month for Wegovy HD 7.2 mg.
- Ozempic copay card (commercial insurance, Novo Nordisk): As low as $25/month for eligible commercially insured patients, subject to a maximum savings of $100/month. Government beneficiaries excluded.
- Ozempic self-pay pricing (NovoCare Pharmacy): $199/month for first 2 months (starter doses) through June 30, 2026, then $349/month.
- Zepbound Savings Program (Eli Lilly): Varies; commercial insurance required. Government beneficiaries excluded.
- Mounjaro Savings Program (Eli Lilly): Varies; commercial insurance required.
Important: If the plan uses a copay accumulator, the manufacturer's copay assistance payment will not count toward the patient's deductible or out-of-pocket maximum. The patient will still owe the full cost share after the copay card benefit is exhausted. Ask about accumulator programs during the benefits verification call.
Step 6: Conduct the benefits verification call
Call the pharmacy benefit number on the patient's insurance card. Use this checklist:
Script for the benefits verification call:
- "I'm calling to verify pharmacy benefits for [patient name], DOB [date], member ID [number]."
- "I need to check coverage for [drug name, strength, dosage form]. The NDC is [number] if needed."
- "Is this medication on the plan's formulary? What tier is it on?"
- "Does it require prior authorization? If so, what are the PA criteria?"
- "Is step therapy required? What drug must be tried first?"
- "Is there a mandatory specialty pharmacy? If so, which one?"
- "What is the patient's copay or coinsurance for this drug?"
- "Is the drug subject to the deductible? How much of the deductible has been met?"
- "Is there a copay accumulator or copay maximizer program on this plan?"
- "What is the PA fax number or electronic submission pathway?"
- "What is the expected turnaround time for PA?"
- "Is there a quantity limit or dose limit for this drug?"
Document every answer, the representative's name, the reference number for the call, and the date and time. This documentation becomes the evidence base if a subsequent PA or claim is denied.
Step 7: Interpret and act on the results
Scenario A: Drug on formulary, PA required, specialty pharmacy identified
→ Submit PA with required documentation → Route prescription to designated specialty pharmacy → If approved, patient receives medication through specialty pharmacy
Scenario B: Drug on formulary, PA required, but step therapy not met
→ Follow the GLP-1 step therapy exception workflow (see companion article) → Document contraindication, intolerance, or therapeutic failure → Submit step therapy exception with PA
Scenario C: Drug not on formulary
→ Request a formulary exception (non-formulary exception request) → Provide clinical rationale for why the specific GLP-1 is medically necessary → If denied, consider prescribing the formulary-preferred GLP-1
Scenario D: Benefit exclusion
→ Verify whether the exclusion applies to the specific indication (obesity vs. T2D vs. MACE risk reduction) → Some plans exclude GLP-1s for obesity but cover the same drug for diabetes or cardiovascular indications → If the patient has a qualifying comorbid condition (e.g., T2D, MACE history), prescribe the GLP-1 under the covered indication → If no covered indication applies, explore manufacturer direct-to-consumer programs (NovoCare Pharmacy, LillyDirect) or patient assistance programs
Scenario E: Plan covers GLP-1 for T2D but not for weight loss
→ If the patient has type 2 diabetes, prescribe the GLP-1 under the T2D indication (Ozempic, Mounjaro, Trulicity) → Wegovy and Zepbound are labeled for weight management, not T2D, so they would not be covered under a T2D-only benefit → Ozempic is labeled for T2D and has weight-loss effects; this is the most common workaround for patients with T2D who want GLP-1 access on weight-loss-restrictive plans
Common benefit investigation pitfalls
1. Assuming coverage based on plan name
A patient with "UnitedHealthcare" coverage may have a self-funded employer plan that excludes weight-loss GLP-1s, while another UHC patient at a different employer has full coverage. Always verify the specific plan's formulary and benefit election, not just the payer name.
2. Not checking the PBM separately
Medical insurance and pharmacy benefits are often administered by different entities. A patient with Aetna medical coverage may have pharmacy benefits managed by CVS Caremark, Express Scripts, or OptumRx. The GLP-1 formulary and PA requirements are set by the PBM, not the medical insurer. Check the pharmacy benefit manager's formulary, not just the medical plan documents.
3. Missing copay accumulator programs
Copay accumulator and maximizer programs — where manufacturer copay assistance does not count toward the patient's deductible or out-of-pocket maximum — have become increasingly common. A patient who receives a $25 copay with a manufacturer savings card may be surprised when, mid-year, the copay card maximum is reached and the full deductible or coinsurance kicks in. Always ask about accumulator programs during the benefits verification call.
4. Sending the prescription to the wrong pharmacy
If the plan mandates specialty pharmacy dispensing, sending the prescription to a retail pharmacy will result in a point-of-sale rejection. This wastes time and delays therapy initiation. Identify the correct specialty pharmacy during the benefit investigation and route the prescription directly.
5. Not verifying the ICD-10 code alignment
Some plans require specific ICD-10 diagnosis codes on the prescription or PA form. If the prescriber uses an ICD-10 code that doesn't match the plan's PA criteria (e.g., using an obesity code when the plan covers the GLP-1 only for T2D), the claim will be denied. Medi-Cal Rx is implementing mandatory ICD-10 diagnosis codes on all pharmacy claims beginning fall 2026, as reported by the California Medical Association.
Tools for GLP-1 benefit investigation
| Tool | What It Does | Access |
|---|---|---|
| CoverMyMeds | Electronic PA submission, formulary check, step therapy verification | covermymeds.com |
| Surescripts Benefit & Price Intelligence | Real-time formulary and benefit check at point of prescribing | Integrated into most EHRs |
| UHC PreCheck MyScript | Check pharmacy eligibility and PA requirements for UHC members | UHCprovider.com |
| NovoCare formulary finder | Check Wegovy/Ozempic coverage by plan | novomedlink.com |
| LillyDirect coverage check | Check Mounjaro/Zepbound coverage | lillydirect.com |
| Payer provider portals | Formulary search, PA criteria, specialty pharmacy lists | Varies by payer |
| Pharmacy benefit desk call | Full benefits verification including cost share, accumulator status | Phone number on insurance card |
Sources
- IntuitionLabs. The ePA Process for GLP-1 Drugs: A Workflow Guide. 2025. (intuitionlabs.ai)
- IntuitionLabs. Pharmacy vs. Medical Benefit Explained: GLP-1 Coverage. 2025. (intuitionlabs.ai)
- KFF. What to Know About the BALANCE Model for GLP-1s in Medicare and Medicaid. 2026. (kff.org)
- KFF. Medicaid Coverage of and Spending on GLP-1s. 2026. (kff.org)
- Mercer. GLP-1 Considerations for 2026: Your Questions Answered. 2026. (mercer.com)
- Novo Nordisk. Wegovy Prior Authorization Criteria and Form — NovoCare/NovoMedLink. 2026. (novomedlink.com)
- Novo Nordisk. NovoCare Pharmacy — Direct-to-Consumer Pricing. 2026. (novocare.com)
- Surescripts. Electronic Benefit Verification and Prior Authorization Automation. 2026. (surescripts.com)
- Truveris. How Pharmacy Plans Are Managing GLP-1 Coverage in 2025. (truveris.com)
- UHC Provider. Clinical Pharmacy and Specialty Drugs — Prior Authorization Programs. 2026. (uhcprovider.com)
- Shields Health Solutions. Addressing GLP-1 Access and Adherence Challenges with Specialty Pharmacy Solutions. 2025. (shieldshealthsolutions.com)
- CMA. GLP-1 Medications for Weight Loss Will No Longer Be Covered by Medi-Cal. April 2026. (cmadocs.org)
- CMS. Information for Medicare Beneficiaries — Medicare GLP-1 Bridge. 2026. (cms.gov)