On May 15, 2026, the FDA approved fam-trastuzumab deruxtecan-nxki (Enhertu, Daiichi Sankyo/AstraZeneca) for two separate indications in HER2-positive early-stage breast cancer — the drug's first approvals in the curative-intent setting. The neoadjuvant indication covers Stage II or III HER2-positive disease, and the adjuvant indication covers patients with residual invasive disease after trastuzumab-based neoadjuvant therapy.
These approvals move Enhertu from the metastatic-disease space, where it has been available since 2019, into early-stage treatment, where the patient population is larger, the treatment-duration calculus is different, and payer coverage criteria are still being written.
This article focuses on what access teams — payer-facing medical liaisons, hub patient-support staff, and oncology practice billing coordinators — need to navigate the new early-stage indications.
What the FDA approved
Neoadjuvant indication (DESTINY-Breast11)
The FDA approved Enhertu 5.4 mg/kg IV every three weeks for four cycles, followed by four cycles of taxane plus trastuzumab plus pertuzumab (THP), as neoadjuvant treatment for adults with HER2-positive (IHC 3+ or ISH+) Stage II or III breast cancer. The approval was based on the DESTINY-Breast11 phase 3 trial (Harbeck et al., Annals of Oncology 2026), which demonstrated superior pathological complete response (pCR) rates with the Enhertu-then-THP regimen compared to the standard neoadjuvant chemotherapy-plus-HER2-targeted-therapy backbone.
The key access implication: the neoadjuvant indication requires HER2-positive status confirmed by an FDA-authorized companion diagnostic. The FDA simultaneously approved the PATHWAY anti-HER-2/neu (4B5) Rabbit Monoclonal Primary Antibody and the VENTANA HER2 Dual ISH DNA Probe Cocktail for patient selection. Prior authorization criteria will likely require documentation of the specific IHC or ISH test result confirming IHC 3+ or ISH+ status.
Adjuvant indication (DESTINY-Breast05)
The FDA approved Enhertu 5.4 mg/kg IV every three weeks for up to 14 cycles as adjuvant treatment for adults with HER2-positive (IHC 3+ or ISH+) breast cancer who have residual invasive disease following neoadjuvant treatment with trastuzumab (with or without pertuzumab) and taxane-based therapy. The approval was based on the DESTINY-Breast05 phase 3 trial (Loibl et al., New England Journal of Medicine 2026), which demonstrated improved invasive disease-free survival (iDFS) compared to T-DM1 (Kadcyla) in this patient population.
The critical access nuance: the adjuvant label specifies residual invasive disease after trastuzumab-based neoadjuvant treatment. This means prior authorization must document:
- The patient received trastuzumab-based neoadjuvant therapy (with or without pertuzumab)
- Surgical pathology confirmed residual invasive disease in the breast or axillary lymph nodes
- The patient's tumor is HER2-positive (IHC 3+ or ISH+)
This is a narrower population than the neoadjuvant indication and parallels the existing Kadcyla adjuvant-access pathway, which access teams may use as a template.
The label restriction that matters
FiercePharma reported that the adjuvant label precludes patients who received Enhertu before surgery from continuing on Enhertu in the post-operative setting. Specifically, the adjuvant indication covers patients who had residual disease after treatment with trastuzumab (with or without pertuzumab) — not after Enhertu. If a patient receives Enhertu neoadjuvantly and still has residual disease, the approved adjuvant pathway is T-DM1, not continued Enhertu.
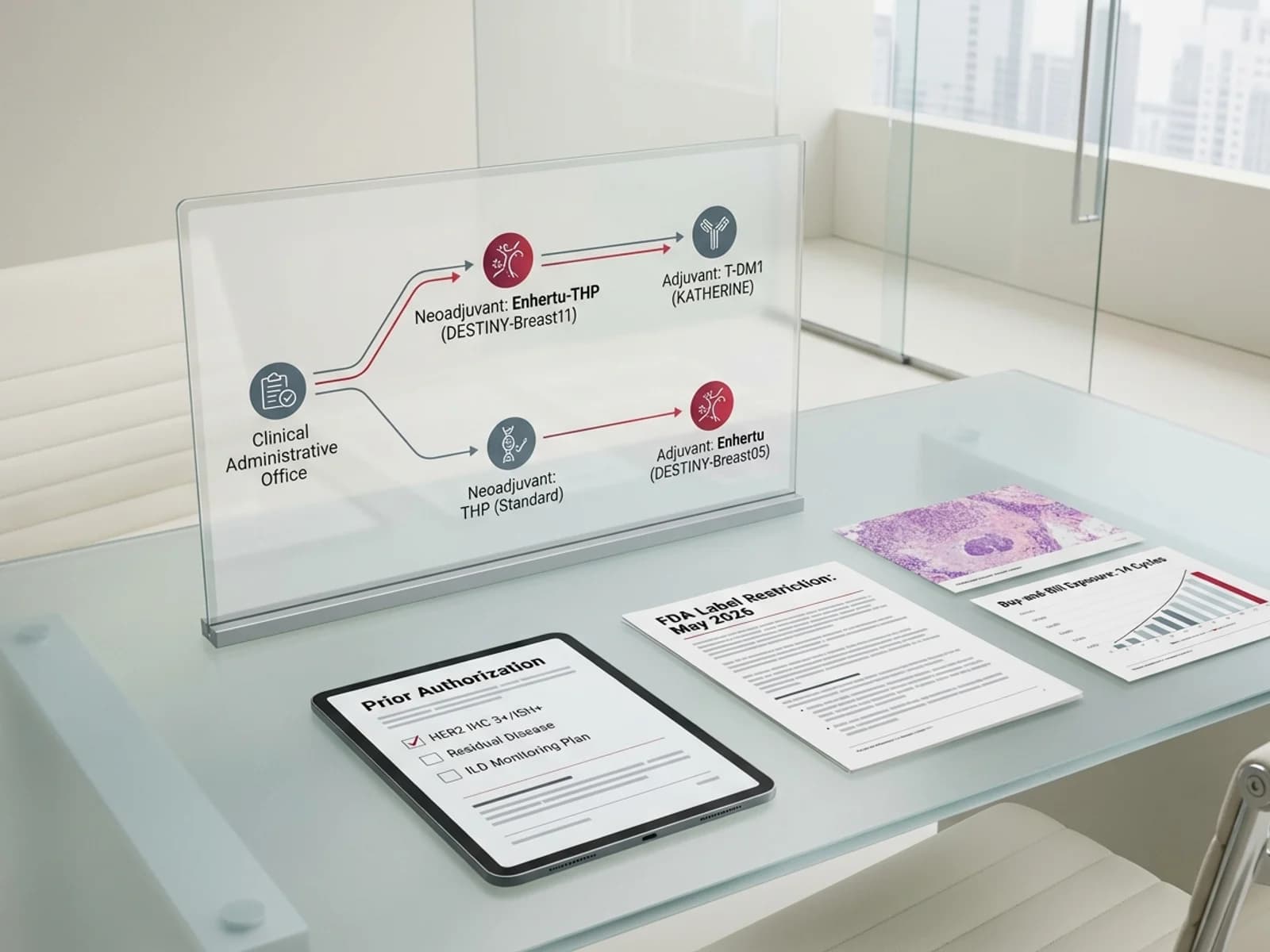
This sequential constraint creates a fork in the treatment algorithm:
- Path A: Enhertu neoadjuvantly → if complete response, proceed to standard adjuvant HER2 therapy. If residual disease, switch to T-DM1 adjuvantly.
- Path B: Standard chemotherapy + trastuzumab/pertuzumab neoadjuvantly → if residual disease, switch to Enhertu adjuvantly.
Payer prior authorization forms will need to account for this sequencing rule.
How this changes prior authorization
New PA criteria that access teams should anticipate
Payers have not yet published finalized PA criteria for the early-stage Enhertu indications, but based on the FDA label and precedent from metastatic-indication PA criteria, access teams should prepare for the following requirements:
Neoadjuvant PA requirements (anticipated):
- Confirmed HER2-positive status: IHC 3+ or ISH+ by FDA-authorized companion diagnostic
- Clinical stage II or III documented by imaging (CT, MRI, or PET-CT) and surgical staging workup
- No prior systemic therapy for the current breast cancer diagnosis (treatment-naive for this cancer episode)
- Prescribed by or in consultation with a medical oncologist
- Treatment facility is an approved infusion site with interstitial lung disease (ILD) monitoring capability
Adjuvant PA requirements (anticipated):
- Confirmed HER2-positive status: IHC 3+ or ISH+
- Prior neoadjuvant trastuzumab-based therapy (with or without pertuzumab) documented
- Surgical pathology report confirming residual invasive disease in the breast or axillary nodes after neoadjuvant therapy
- No prior Enhertu exposure in the neoadjuvant setting (per the label restriction)
- LVEF assessment within normal limits before initiating adjuvant Enhertu
The documentation gap
Oncology practices already navigate HER2 testing, surgical-pathology reporting, and neoadjuvant-treatment documentation for existing adjuvant-therapy PA submissions (Kadcyla, Herceptin). However, the Enhertu early-stage approval introduces new documentation requirements:
- Companion diagnostic specificity — the FDA approved the PATHWAY 4B5 and VENTANA Dual ISH tests specifically for patient selection in the early-stage indications. Some payers may require documentation that the HER2 test was performed using one of these FDA-authorized assays rather than a laboratory-developed test (LDT).
- Residual-disease quantification — the DESTINY-Breast05 trial enrolled patients with high-risk features, including positive node status (ypN1-3) or inoperable presentation. Payers may request documentation of the specific residual-disease characteristics to confirm the patient meets the intended population.
- Trastuzumab exposure documentation — verifying that the patient received trastuzumab-based neoadjuvant therapy (with or without pertuzumab) requires infusion-treatment records, which may not be automatically transmitted between the surgical oncology and medical oncology teams.
Interstitial lung disease monitoring in early-stage patients
Why ILD monitoring is a bigger concern in the curative setting
Enhertu carries a Boxed Warning for interstitial lung disease (ILD) and pneumonitis. In the metastatic setting, the risk-benefit calculus tolerates a higher rate of adverse events because the alternative is disease progression. In the early-stage setting, patients are being treated with curative intent, and the threshold for acceptable toxicity is lower.
DESTINY-Breast11 and DESTINY-Breast05 both required regular ILD monitoring protocols, including baseline CT chest imaging and periodic reassessment. For the neoadjuvant indication (four cycles of Enhertu), the monitoring window is compressed, but for the adjuvant indication (up to 14 cycles), patients may receive Enhertu for nearly a year — a substantially longer exposure duration than in most metastatic trials.
Access teams should anticipate that payers may require:
- Documentation of baseline pulmonary assessment (CT chest or HRCT) before first Enhertu dose
- ILD monitoring plan documented in the treatment summary
- Prescriber attestation that the patient has been counseled on ILD symptoms (cough, dyspnea, fever)
Site-of-care and buy-and-bill considerations
J-code billing for early-stage Enhertu
Enhertu is billed under HCPCS code J9358 (trastuzumab deruxtecan, 1 mg). The same J-code applies across all indications — metastatic, early-stage neoadjuvant, and adjuvant. However, the treatment duration and total dose differ substantially:
- Neoadjuvant: Four cycles at 5.4 mg/kg = approximately 4–5 vials per cycle for an average-weight patient, for a total of 16–20 vials over the neoadjuvant course
- Adjuvant: Up to 14 cycles at 5.4 mg/kg = approximately 56–70 vials over the full adjuvant course
The adjuvant course represents a significantly larger drug-volume commitment than any previous Enhertu indication. For buy-and-bill practices, the inventory-carrying cost and reimbursement-timing risk increase proportionally. Practices that already stock Enhertu for metastatic patients may need to increase their order volume and adjust their revenue-cycle-management processes to accommodate the longer treatment duration.
Inventory and reimbursement risk
The total adjuvant course cost at 5.4 mg/kg for a 70-kg patient over 14 cycles is substantially higher than the metastatic cost per patient, because metastatic treatment often continues until disease progression (which may be sooner than 14 cycles) or unacceptable toxicity, while the adjuvant course has a fixed maximum duration. Practices should model the acquisition-cost exposure and ensure that their accounts-receivable processes can handle the extended reimbursement timeline.
Competitive landscape: Enhertu vs. Kadcyla in early-stage
The Kadcyla adjuvant displacement question
Prior to the Enhertu approval, a common guideline-backed adjuvant option for HER2-positive patients with residual invasive disease after neoadjuvant therapy was T-DM1 (Kadcyla, Roche), based on the KATHERINE trial. The DESTINY-Breast05 trial directly compared Enhertu to T-DM1 in this population and demonstrated superior invasive disease-free survival.
From an access perspective, the Enhertu vs. Kadcyla dynamic will play out in:
- Formulary decision-making — payers that currently prefer Kadcyla on formulary will need to evaluate whether to add Enhertu, prefer Enhertu, or maintain Kadcyla with step-therapy requirements
- Step-therapy protocols — some payers may initially require a trial of Kadcyla before approving Enhertu, citing the longer real-world experience with Kadcyla. Access teams should prepare appeals documentation demonstrating the DESTINY-Breast05 efficacy advantage
- Cost considerations — Kadcyla and Enhertu are both expensive antibody-drug conjugates. Payers will evaluate the relative cost-effectiveness of each, factoring in the iDFS benefit demonstrated in DESTINY-Breast05
Neoadjuvant landscape shift
In the neoadjuvant setting, Enhertu enters a treatment paradigm where chemotherapy plus trastuzumab and pertuzumab has been the backbone for years. The DESTINY-Breast11 trial showed that four cycles of single-agent Enhertu followed by THP produced superior pCR rates compared to the chemotherapy-plus-THP regimen. This positions Enhertu as an important new neoadjuvant option, but adoption will depend on payer coverage, ILD monitoring infrastructure, and prescriber familiarity with the ADC in the pre-surgical setting.
What access teams should do now
- Update HER2 testing workflows — confirm that the pathology labs your practice uses offer the FDA-authorized PATHWAY 4B5 and/or VENTANA Dual ISH tests. If your lab uses an LDT, check with major payers whether they accept LDT results for Enhertu early-stage PA.
- Prepare surgical-pathology documentation templates — for the adjuvant indication, ensure that surgical-pathology reports explicitly document residual invasive disease, nodal status, and HER2 results. Create a standardized cover sheet for PA submissions that includes all required documentation elements.
- Establish ILD monitoring protocols — develop a baseline-CT and follow-up-monitoring protocol that meets both the Enhertu prescribing information and anticipated payer requirements.
- Model buy-and-bill exposure — for practices that bill under the buy-and-bill model, calculate the per-patient inventory cost for a full 14-cycle adjuvant course and ensure revenue-cycle processes can handle the extended reimbursement timeline.
- Monitor payer criteria publication — major payers (CVS Caremark, Express Scripts, Optum Rx) and Medicare Part D plan sponsors will publish PA criteria for the new indications in the coming months. Track these criteria as they are released and update your PA submission templates accordingly.
- Prepare appeal templates — for patients who are denied Enhertu in favor of Kadcyla, prepare an appeal template that cites the DESTINY-Breast05 iDFS data, the FDA-approved indication, and the NCCN guideline recommendation (once updated).
Sources
- FDA, "FDA approves two separate indications for fam-trastuzumab deruxtecan-nxki in HER2-positive early-stage breast cancer" — https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-two-separate-indications-fam-trastuzumab-deruxtecan-nxki-her2-positive-early-stage
- AstraZeneca, "Enhertu approved in the US for two new indications for patients with HER2-positive early breast cancer" — https://www.astrazeneca.com/media-centre/press-releases/2026/enhertu-approved-in-two-her2-early-bc-settings.html
- Harbeck N, Modi S, Pusztai L, et al. "Neoadjuvant trastuzumab deruxtecan alone or followed by paclitaxel, trastuzumab, and pertuzumab for high-risk HER2-positive early breast cancer (DESTINY-Breast11)." Ann Oncol. 2026;37(2):166-179.
- Loibl S, et al. "Trastuzumab deruxtecan in residual HER2-positive early breast cancer." N Engl J Med. 2026;394(9):845-857.
- Daiichi Sankyo, "ENHERTU prescribing information, revised May 2026" — https://www.accessdata.fda.gov/drugsatfda_docs/label/2026/761139s030lbl.pdf
- FiercePharma, "Daiichi, AstraZeneca's Enhertu breaks into early breast cancer with dual FDA approvals" — https://www.fiercepharma.com/pharma/daiichi-astrazeneca-enhertu-breaks-early-breast-cancer-dual-fda-approvals
- Breast Cancer Research Foundation, "FDA Approves Metastatic Breast Cancer Drug Enhertu for Early-Stage Disease" — https://www.bcrf.org/blog/fda-approves-enhertu-for-early-stage-breast-cancer